

Association Between Long-term Exposure to Ambient Air Pollution and Change in Quantitatively Assessed Emphysema and Lung Function
- PMID: 31408135
- PMCID: PMC6692674
- DOI: 10.1001/jama.2019.10255
Association Between Long-term Exposure to Ambient Air Pollution and Change in Quantitatively Assessed Emphysema and Lung Function
Abstract
Importance: While air pollutants at historical levels have been associated with cardiovascular and respiratory diseases, it is not known whether exposure to contemporary air pollutant concentrations is associated with progression of emphysema.
Objective: To assess the longitudinal association of ambient ozone (O3), fine particulate matter (PM2.5), oxides of nitrogen (NOx), and black carbon exposure with change in percent emphysema assessed via computed tomographic (CT) imaging and lung function.
Design, setting, and participants: This cohort study included participants from the Multi-Ethnic Study of Atherosclerosis (MESA) Air and Lung Studies conducted in 6 metropolitan regions of the United States, which included 6814 adults aged 45 to 84 years recruited between July 2000 and August 2002, and an additional 257 participants recruited from February 2005 to May 2007, with follow-up through November 2018.
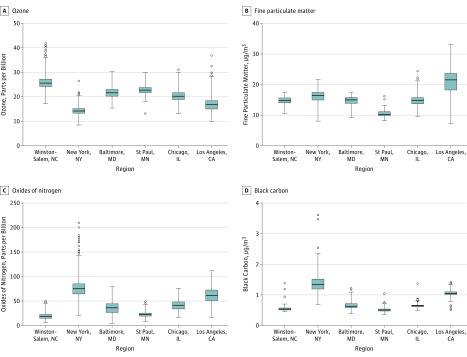
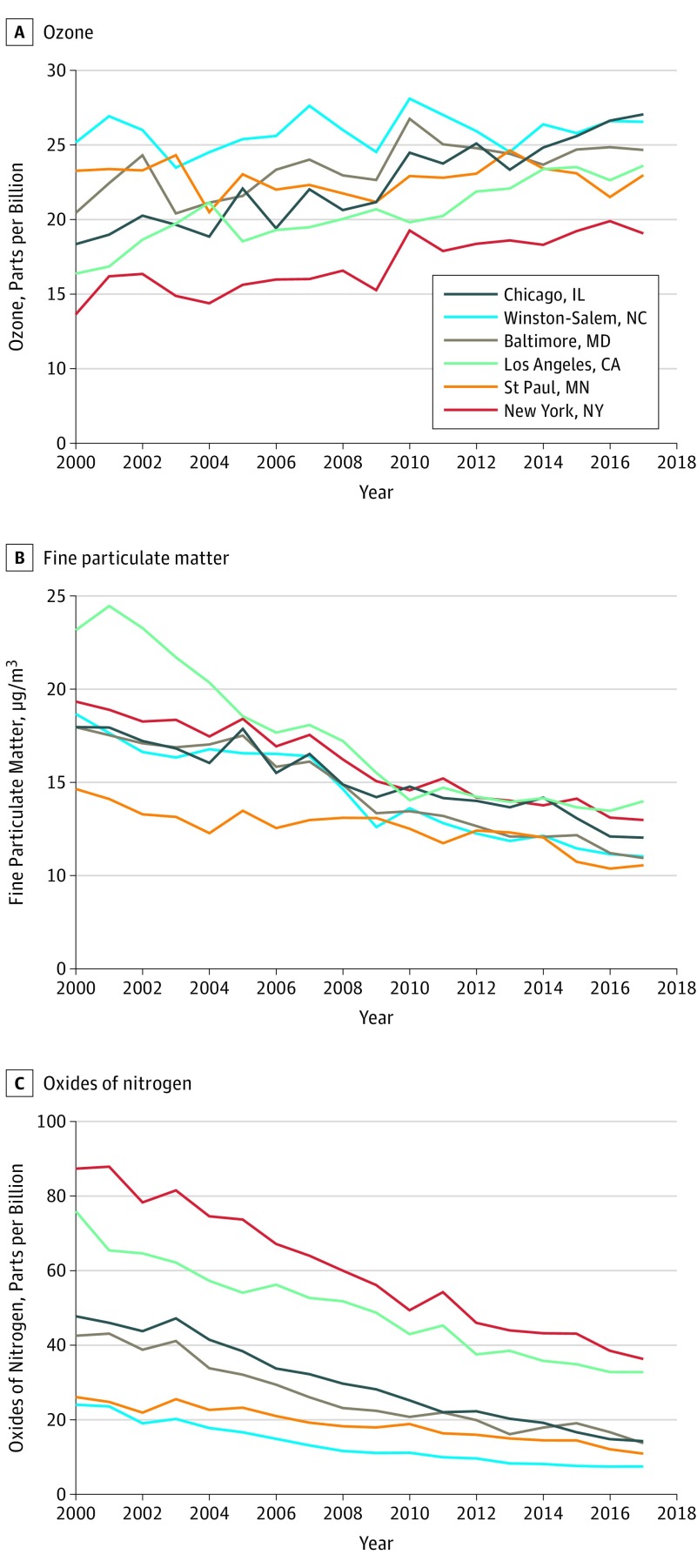
Exposures: Residence-specific air pollutant concentrations (O3, PM2.5, NOx, and black carbon) were estimated by validated spatiotemporal models incorporating cohort-specific monitoring, determined from 1999 through the end of follow-up.
Main outcomes and measures: Percent emphysema, defined as the percent of lung pixels less than -950 Hounsfield units, was assessed up to 5 times per participant via cardiac CT scan (2000-2007) and equivalent regions on lung CT scans (2010-2018). Spirometry was performed up to 3 times per participant (2004-2018).
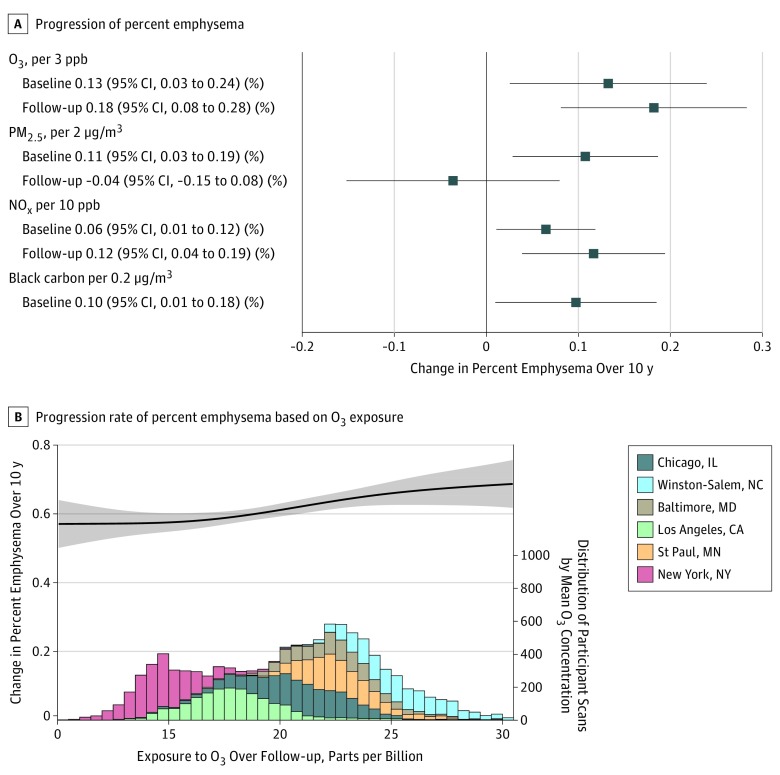
Results: Among 7071 study participants (mean [range] age at recruitment, 60 [45-84] years; 3330 [47.1%] were men), 5780 were assigned outdoor residential air pollution concentrations in the year of their baseline examination and during the follow-up period and had at least 1 follow-up CT scan, and 2772 had at least 1 follow-up spirometric assessment, over a median of 10 years. Median percent emphysema was 3% at baseline and increased a mean of 0.58 percentage points per 10 years. Mean ambient concentrations of PM2.5 and NOx, but not O3, decreased substantially during follow-up. Ambient concentrations of O3, PM2.5, NOx, and black carbon at study baseline were significantly associated with greater increases in percent emphysema per 10 years (O3: 0.13 per 3 parts per billion [95% CI, 0.03-0.24]; PM2.5: 0.11 per 2 μg/m3 [95% CI, 0.03-0.19]; NOx: 0.06 per 10 parts per billion [95% CI, 0.01-0.12]; black carbon: 0.10 per 0.2 μg/m3 [95% CI, 0.01-0.18]). Ambient O3 and NOx concentrations, but not PM2.5 concentrations, during follow-up were also significantly associated with greater increases in percent emphysema. Ambient O3 concentrations, but not other pollutants, at baseline and during follow-up were significantly associated with a greater decline in forced expiratory volume in 1 second per 10 years (baseline: 13.41 mL per 3 parts per billion [95% CI, 0.7-26.1]; follow-up: 18.15 mL per 3 parts per billion [95% CI, 1.59-34.71]).
Conclusions and relevance: In this cohort study conducted between 2000 and 2018 in 6 US metropolitan regions, long-term exposure to ambient air pollutants was significantly associated with increasing emphysema assessed quantitatively using CT imaging and lung function.
Conflict of interest statement
Figures

Comment in
-
Air Pollution Associated with Emphysema, Worsening Lung Function.Am J Nurs. 2019 Dec;119(12):58. doi: 10.1097/01.NAJ.0000615800.17409.8d. Am J Nurs. 2019. PMID: 31764054 No abstract available.
References
-
- Kochanek KD, Murphy SL, Xu JQ, Arias E. Mortality in the United States, 2016. NCHS Data Brief, No. 293. Hyattsville, MD: National Center for Health Statistics; 2017. - PubMed
-
- GBD 2017 Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736-1788. doi:10.1016/S0140-6736(18)32203-7 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- RC1 HL100543/HL/NHLBI NIH HHS/United States
- S10 OD018526/OD/NIH HHS/United States
- R01 HL112986/HL/NHLBI NIH HHS/United States
- K23 HL141651/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- R01 ES023500/ES/NIEHS NIH HHS/United States
- R01 HL155816/HL/NHLBI NIH HHS/United States
- R01 HL130506/HL/NHLBI NIH HHS/United States
- K24 ES013195/ES/NIEHS NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- P30 ES007033/ES/NIEHS NIH HHS/United States
- R01 HL121270/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
