

Association of Midlife to Late-Life Blood Pressure Patterns With Incident Dementia
- PMID: 31408138
- PMCID: PMC6692677
- DOI: 10.1001/jama.2019.10575
Association of Midlife to Late-Life Blood Pressure Patterns With Incident Dementia
Abstract
Importance: The association between late-life blood pressure (BP) and cognition may depend on the presence and chronicity of past hypertension. Late-life declines in blood pressure following prolonged hypertension may be associated with poor cognitive outcomes.
Objective: To examine the association of midlife to late-life BP patterns with subsequent dementia, mild cognitive impairment, and cognitive decline.
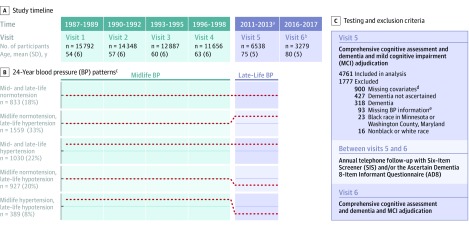
Design, setting, and participants: The Atherosclerosis Risk in Communities prospective population-based cohort study enrolled 4761 participants during midlife (visit 1, 1987-1989) and followed-up over 6 visits through 2016-2017 (visit 6). BP was examined over 24 years at 5 in-person visits between visits 1 and 5 (2011-2013). During visits 5 and 6, participants underwent detailed neurocognitive evaluation. The setting was 4 US communities: Washington County, Maryland; Forsyth County, North Carolina; Jackson, Mississippi; and Minneapolis, Minnesota. Follow-up ended on December 31, 2017.
Exposures: Five groups based on longitudinal patterns of normotension, hypertension (>140/90 mm Hg), and hypotension (<90/60 mm Hg) at visits 1 to 5.
Main outcomes and measures: Primary outcome was dementia onset after visit 5, based on Ascertain Dementia-8 informant questionnaires, Six-Item Screener telephone assessments, hospital discharge and death certificate codes, and the visit 6 neurocognitive evaluation. Secondary outcome was mild cognitive impairment at visit 6, based on the neurocognitive evaluation.
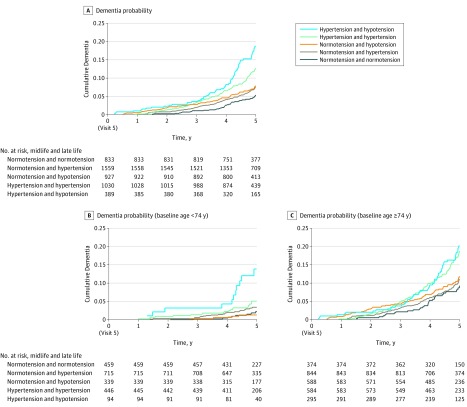
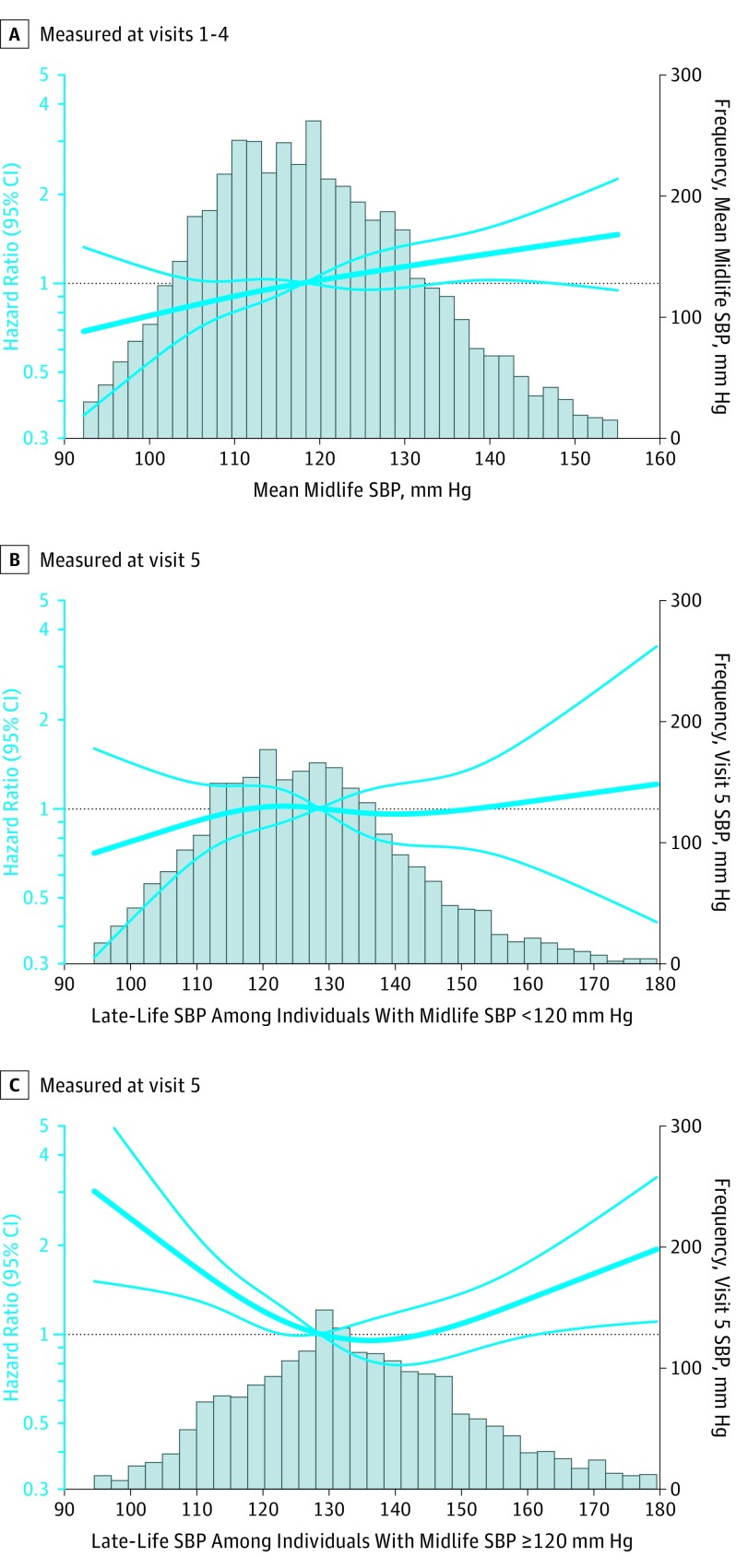
Results: Among 4761 participants (2821 [59%] women; 979 [21%] black race; visit 5 mean [SD] age, 75 [5] years; visit 1 mean age range, 44-66 years; visit 5 mean age range, 66-90 years), there were 516 (11%) incident dementia cases between visits 5 and 6. The dementia incidence rate for participants with normotension in midlife (n = 833) and late life was 1.31 (95% CI, 1.00-1.72 per 100 person-years); for midlife normotension and late-life hypertension (n = 1559), 1.99 (95% CI, 1.69-2.32 per 100 person-years); for midlife and late-life hypertension (n = 1030), 2.83 (95% CI, 2.40-3.35 per 100 person-years); for midlife normotension and late-life hypotension (n = 927), 2.07 (95% CI, 1.68-2.54 per 100 person-years); and for midlife hypertension and late-life hypotension (n = 389), 4.26 (95% CI, 3.40-5.32 per 100 person-years). Participants in the midlife and late-life hypertension group (hazard ratio [HR], 1.49 [95% CI, 1.06-2.08]) and in the midlife hypertension and late-life hypotension group (HR, 1.62 [95% CI, 1.11-2.37]) had significantly increased risk of subsequent dementia compared with those who remained normotensive. Irrespective of late-life BP, sustained hypertension in midlife was associated with dementia risk (HR, 1.41 [95% CI, 1.17-1.71]). Compared with those who were normotensive in midlife and late life, only participants with midlife hypertension and late-life hypotension had higher risk of mild cognitive impairment (37 affected individuals (odds ratio, 1.65 [95% CI, 1.01-2.69]). There was no significant association of BP patterns with late-life cognitive change.
Conclusions and relevance: In this community-based cohort with long-term follow-up, sustained hypertension in midlife to late life and a pattern of midlife hypertension and late-life hypotension, compared with midlife and late-life normal BP, were associated with increased risk for subsequent dementia.
Conflict of interest statement
Figures
Comment in
-
Blood Pressure, Brain Volume and White Matter Hyperintensities, and Dementia Risk.JAMA. 2019 Aug 13;322(6):512-513. doi: 10.1001/jama.2019.10849. JAMA. 2019. PMID: 31408120 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
