

Dermatologists' perceptions on the utility and limitations of teledermatology after examining 55,000 lesions
- PMID: 31409225
- PMCID: PMC8044615
- DOI: 10.1177/1357633X19864829
Dermatologists' perceptions on the utility and limitations of teledermatology after examining 55,000 lesions
Abstract
Introduction: Few studies have assessed the perception of teledermatologists about the utility and limitations of teledermatology, especially to diagnose a broad range of skin diseases. This study aimed to evaluate dermatologists' confidence in teledermatology, its utility and limitations for dermatological conditions in primary care.
Methods: An analytical study that used a survey for dermatologists who diagnosed 30,916 patients with 55,012 lesions through teledermatology during a 1-year project in São Paulo, Brazil.
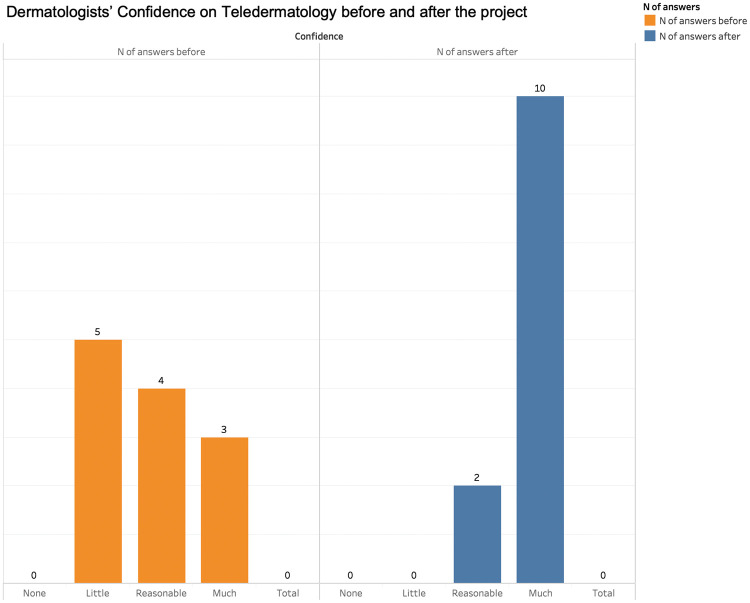
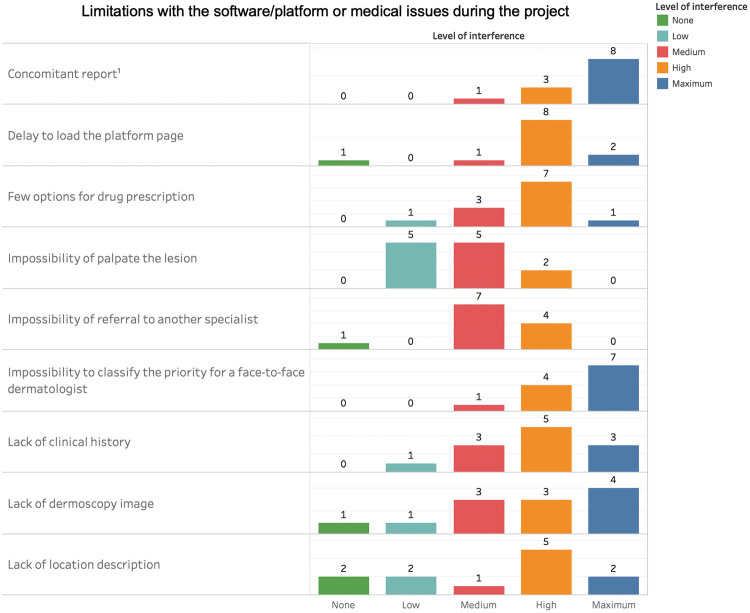
Results: Dermatologists found teledermatology useful for triage and diagnosis, especially for xerotic eczema, pigmentary disorders and superficial infections. Their confidence in teledermatology was statistically higher by the end of the project (p = 0.0012). Limitations included some technical issues and the impossibility to suggest how soon the patient should be assisted face-to-face by a dermatologist. The most treatable group of diseases by teledermatology was superficial infections (92%). The use of dermoscopy images would significantly increase the confidence to treat atypical naevi and malignant tumours (p < 0.0001 and p = 0.0003 respectively). Follow-ups by teledermatology or feedback from primary-care physicians would be desirable, according to the dermatologists.
Discussion: We found it interesting that dermatologists became increasingly confident in teledermatology after the project and how they classified teledermatology as useful for triage, diagnosis and even treatment of most types of skin conditions followed at primary care. Dermoscopy should definitely be added to the photographs, especially for malignant tumours and atypical naevi. Most of the technical limitations found could be solved with a few improvements in the software/platform.
Keywords: Teledermatology; dermatologist; limitations; survey; utility.
Conflict of interest statement
Figures



References
-
- Wurm EM, Hofmann-Wellenhof R, Wurm R, et al. Telemedicine and teledermatology: Past, present and future. J Dtsch Dermatol Ges 2008; 6: 106–112. - PubMed
-
- Pathipati AS, Lee L, Armstrong AW. Health-care delivery methods in teledermatology: Consultative, triage and direct-care models. J Telemed Telecare 2011; 17: 214–216. - PubMed
-
- Loane MA, Gore HE, Bloomer SE, et al. Preliminary results from the Northern Ireland arms of the UK Multicentre Teledermatology Trial: Is clinical management by realtime teledermatology possible? J Telemed Telecare 1998; 4 Suppl 1: 3–5. - PubMed
-
- Ferrándiz L, Ruiz-de-Casas A, Martin-Gutierrez FJ, et al. Effect of teledermatology on the prognosis of patients with cutaneous melanoma. Arch Dermatol 2012; 148: 1025–1028. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
