

360° ab-interno Schlemm's canal viscodilation in primary open-angle glaucoma
- PMID: 31409962
- PMCID: PMC6645607
- DOI: 10.2147/OPTH.S203917
360° ab-interno Schlemm's canal viscodilation in primary open-angle glaucoma
Abstract
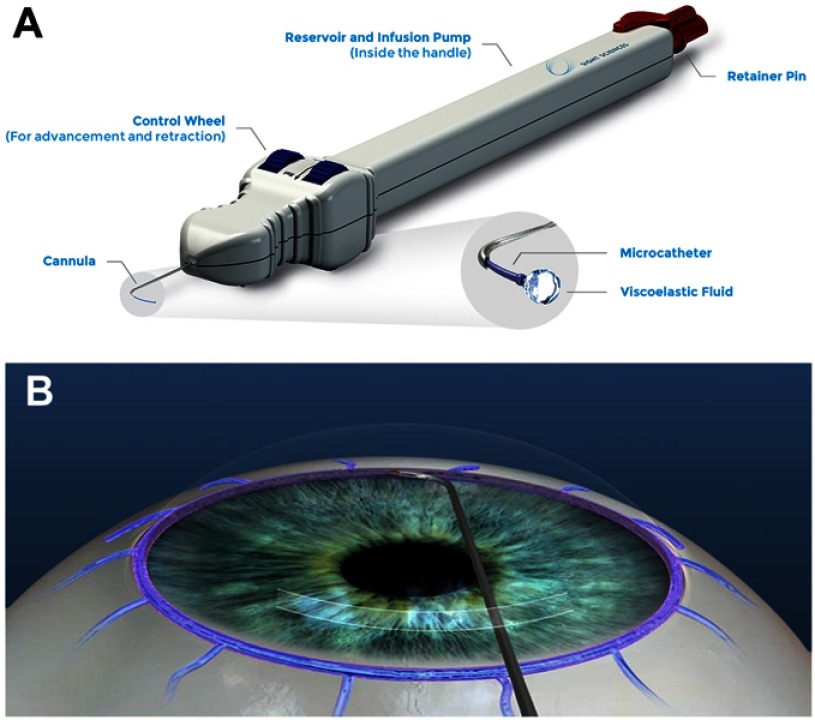
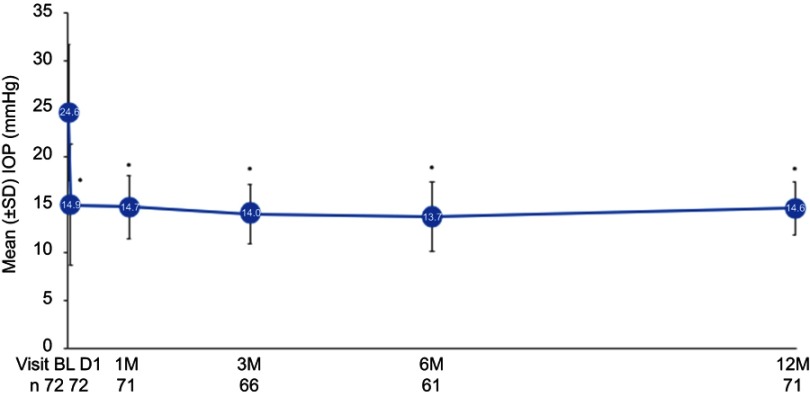
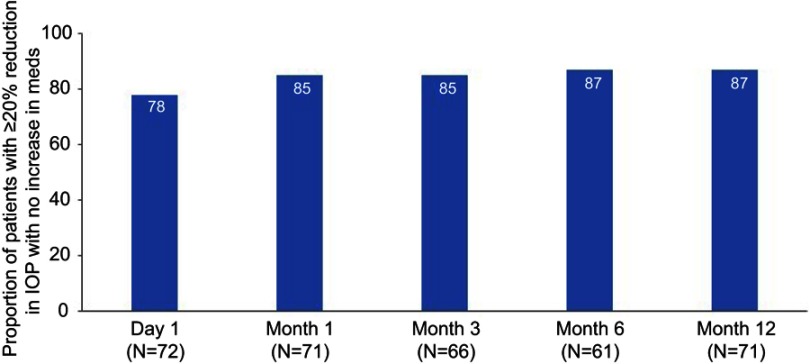
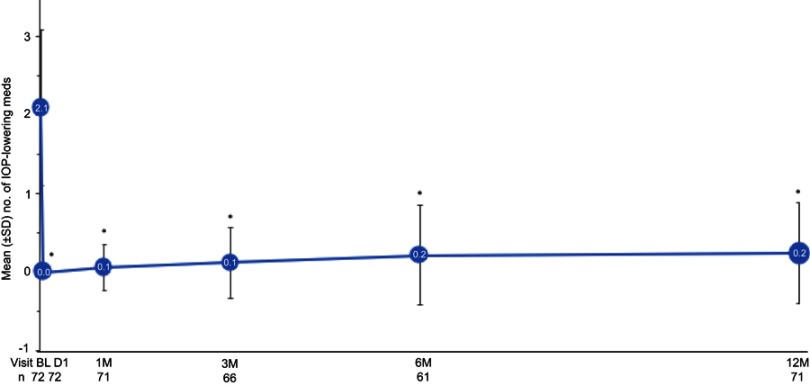
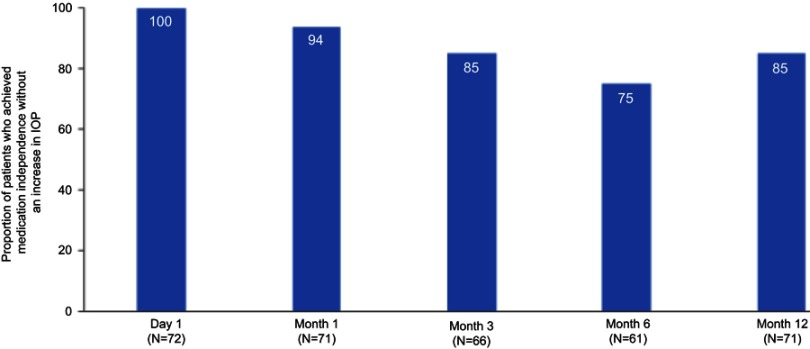
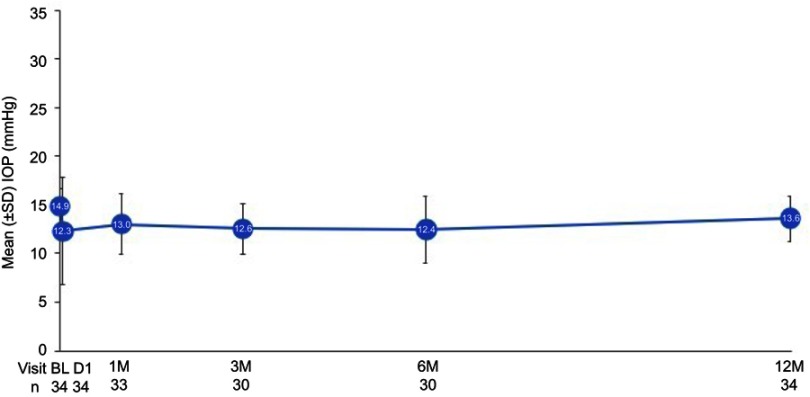
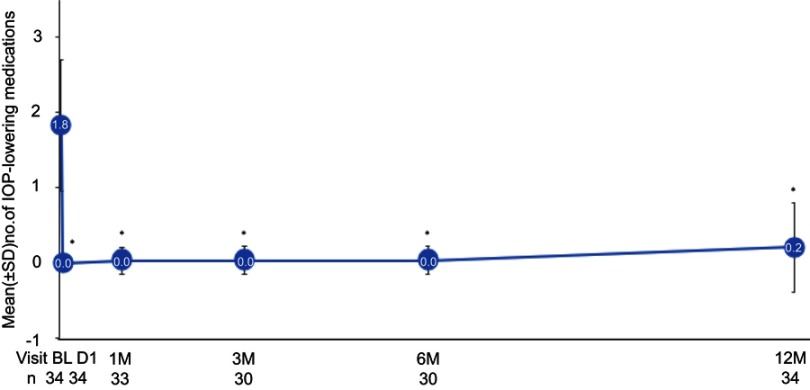
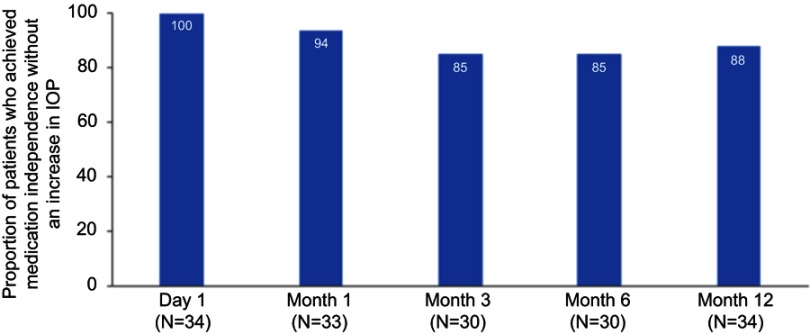
Purpose: To evaluate the safety and effectiveness of ab-interno microcatheterization and 360° viscodilation of Schlemm's canal (SC) using the VISCO360® Viscosurgical System in treatment of primary open angle glaucoma (POAG). Setting: Surgical center (Augencentrum Köln, Köln, Germany). Design: Retrospective analysis of 106 eyes from 71 consecutive patients. Methods: Ab-interno canal viscodilation (VISCO360®) with or without cataract extraction was performed in two groups of patients with mild-moderate POAG: Group 1 had a baseline intraocular pressure (IOP) ≥18 mmHg (n=72 eyes) and Group 2 had a baseline IOP <18 mmHg (n=34 eyes). IOP without washout was measured and number of IOP-lowering medications were documented at all visits. Effectiveness was determined by reduction in IOP and reduction in the number of IOP-lowering medications at 12±3 months from baseline. Safety was determined by the rate of adverse events (AEs) and secondary surgical interventions (SSI). Results: In Group 1, all eyes available at 12±3 months (n=72), had a 41.0% reduction in mean IOP (from 24.6±7.1 mmHg to 14.6±2.8 mmHg), 87% (n=62) of which showed an IOP reduction of ≥20% with no increase in IOP-lowering medications. In Group 2, all eyes (n=34) maintained their baseline IOP at all postoperative visits. In both groups, a significant decrease (>89%) in mean number of IOP-lowering medications was seen at 12 months with 86% of eyes completely off medication with no increase in IOP. The most common AE seen was hyphema (13%) and no eye required SSI during the study period. Conclusion: Ab-interno SC viscodilation (VISCO360) is safe and effective in lowering IOP and reducing hypotensive medications in patients with OAG.
Keywords: 360-degree trabeculotomy; POAG; VISCO360®; blebless, MIGS; canaloplasty.
Conflict of interest statement
The authors have no commercial or proprietary interest in any of the materials discussed in this article. The authors report no conflicts of interest in this work.
Figures

References
-
- Stegmann R. Visco-canalostomy: a new surgical technique for open angle glaucoma. Ann de Istituto Barraquer. 1995;25:229–232.
LinkOut - more resources
Full Text Sources
