

Idiopathic epiretinal membrane surgery: safety, efficacy and patient related outcomes
- PMID: 31409964
- PMCID: PMC6643061
- DOI: 10.2147/OPTH.S176120
Idiopathic epiretinal membrane surgery: safety, efficacy and patient related outcomes
Abstract
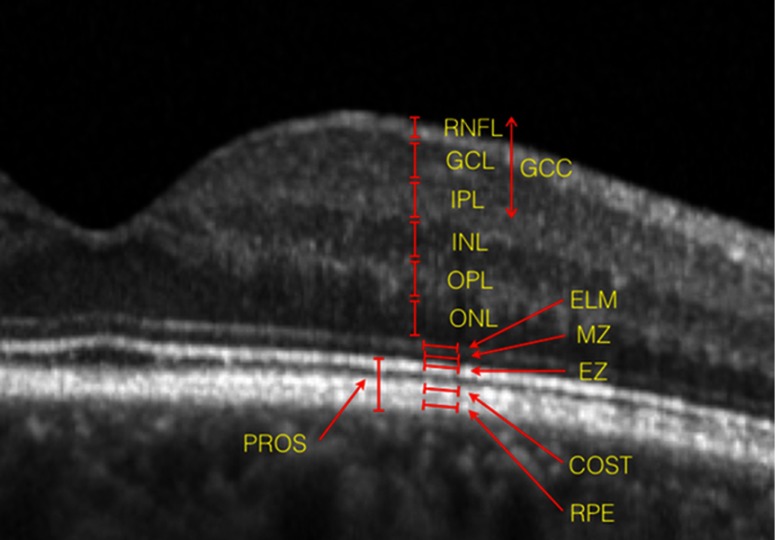
This review aims to give to the reader an overview selectively oriented on safety and efficacy of surgery, providing concise and direct answers about crucial questions of trainees and experts. Surgery for idiopathic epiretinal membrane (ERM) is a safe and effective procedure that can achieve long-term stable postoperative visual and anatomical improvement, with an overall low recurrence and complication rate. Young patients, with a short onset of symptoms and with better initial visual acuity achieve higher levels of visual outcome. The preoperative degree of metamorphopsia is the prognostic factor for their postoperative degree. Successful results may be obtained in eyes with specific optical coherence tomography criteria, such as thin ganglion cell layers, thin internal plexiform layer, longer photoreceptors outer segment, regular ellipsoid zone and cone outer segment tips line, and without ectopic inner foveal layer. Internal limiting membrane peeling demonstrates positive anatomical and functional outcomes, but final positions about its safety remain controversial.
Keywords: efficacy; idiopathic epiretinal membrane; outcome; prognostic factor; safety.
Conflict of interest statement
Professor Francesco Bandello reports personal fees from Allergan, Bayer, Boehringer-Ingelheim, Fidia Sooft, Hofmann La Roche, Novartis, NTC Pharma, Sifi, Thrombogenics, and Zeiss, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- Melberg NS, Thomas MA. Nuclear sclerotic cataract after vitrectomy in patients younger than 50 years of age. Ophthalmology. 1995;102(10):1466–1471. - PubMed
LinkOut - more resources
Full Text Sources
