

Prognostic accuracy of SOFA, qSOFA and SIRS criteria in hematological cancer patients: a retrospective multicenter study
- PMID: 31410290
- PMCID: PMC6686367
- DOI: 10.1186/s40560-019-0396-y
Prognostic accuracy of SOFA, qSOFA and SIRS criteria in hematological cancer patients: a retrospective multicenter study
Abstract
Background: With Sepsis-3, the increase in sequential organ failure assessment (SOFA) as a clinical score for the identification of patients with sepsis and quickSOFA (qSOFA) for the identification of patients at risk of sepsis outside the intensive care unit (ICU) were introduced in 2016. However, their validity has been questioned, and their applicability in different settings and subgroups, such as hematological cancer patients, remains unclear. We therefore assessed the validity of SOFA, qSOFA, and the systemic inflammatory response syndrome (SIRS) criteria regarding the diagnosis of sepsis and the prediction of in-hospital mortality in a multicenter cohort of hematological cancer patients treated on ICU and non-ICU settings.
Methods: We retrospectively calculated SIRS, SOFA, and qSOFA scores in our cohort and applied the definition of sepsis as "life-threatening organ dysfunction caused by dysregulated host response to infection" as reference. Discriminatory capacity was assessed using the area under the receiver operating characteristic curve (AUROC).
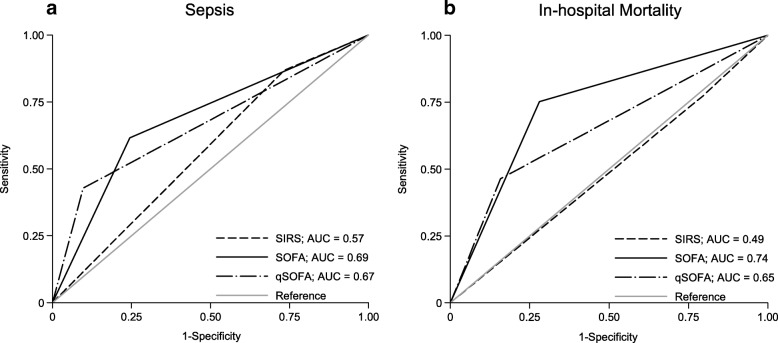
Results: Among 450 patients with hematological cancer (median age 58 years, 274 males [61%]), 180 (40%) had sepsis of which 101 (56%) were treated on ICU. For the diagnosis of sepsis, sensitivity was 86%, 64%, and 42% for SIRS, SOFA, and qSOFA, respectively. However, the AUROCs of SOFA and qSOFA indicated better discrimination for sepsis than SIRS (SOFA, 0.69 [95% CI, 0.64-0.73] p < 0.001; qSOFA, 0.67 [95% CI, 0.62-0.71] p < 0.001; SIRS, 0.57 [95% CI, 0.53-0.61] p < 0.001).In-hospital mortality was 40% and 14% in patients with and without sepsis, respectively (p < 0.001). Regarding patients with sepsis, mortality was similar in patients with positive and negative SIRS scores (39% vs. 40% (p = 0.899), respectively). For patients with qSOFA ≥ 2, mortality was 49% compared to 33% for those with qSOFA < 2 (p = 0.056), and for SOFA 56% vs. 11% (p < 0.001), respectively. SOFA allowed significantly better discrimination for in-hospital mortality (AUROC 0.74 [95% CI, 0.69-0.79] p < 0.001) than qSOFA (AUROC 0.65 [95% CI, 0.60-0.71] p < 0.001) or SIRS (AUROC 0.49 [95% CI, 0.44-0.54] p < 0.001).
Conclusions: An increase in SOFA score of ≥ 2 had better prognostic accuracy for both diagnosis of sepsis and in-hospital mortality in this setting, and especially on ICU, we observed limited validity of SIRS criteria and qSOFA in identifying hematological patients with sepsis and at high risk of death.
Keywords: Cancer; Hematological malignancies; SIRS; Sepsis; Sepsis-3; qSOFA.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures
References
-
- Shankar-Hari M, Phillips GS, Levy ML, Seymour CW, Liu VX, Deutschman CS, et al. Developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for sepsis and septic shock (Sepsis-3) JAMA. 2016;315(8):775–787. doi: 10.1001/jama.2016.0289. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
