

EANM guideline for ventilation/perfusion single-photon emission computed tomography (SPECT) for diagnosis of pulmonary embolism and beyond
- PMID: 31410539
- PMCID: PMC6813289
- DOI: 10.1007/s00259-019-04450-0
EANM guideline for ventilation/perfusion single-photon emission computed tomography (SPECT) for diagnosis of pulmonary embolism and beyond
Abstract
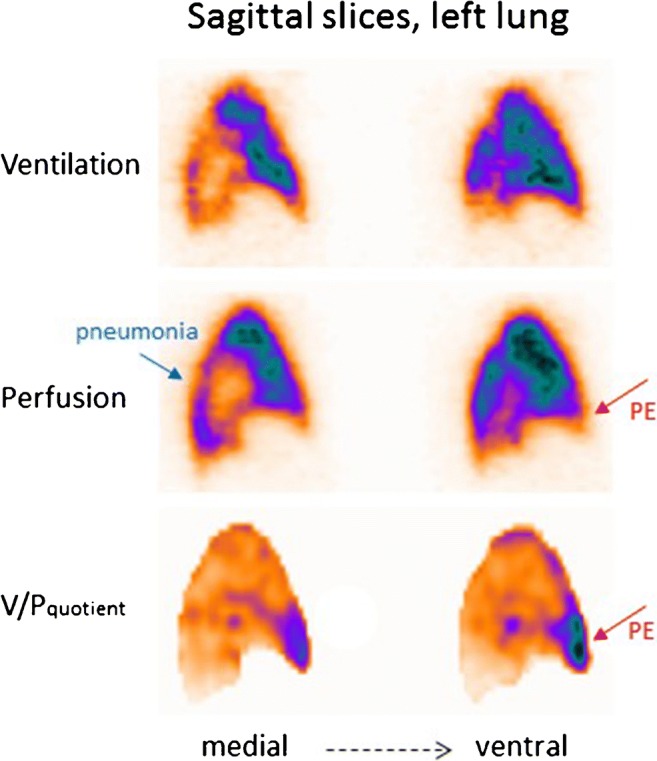
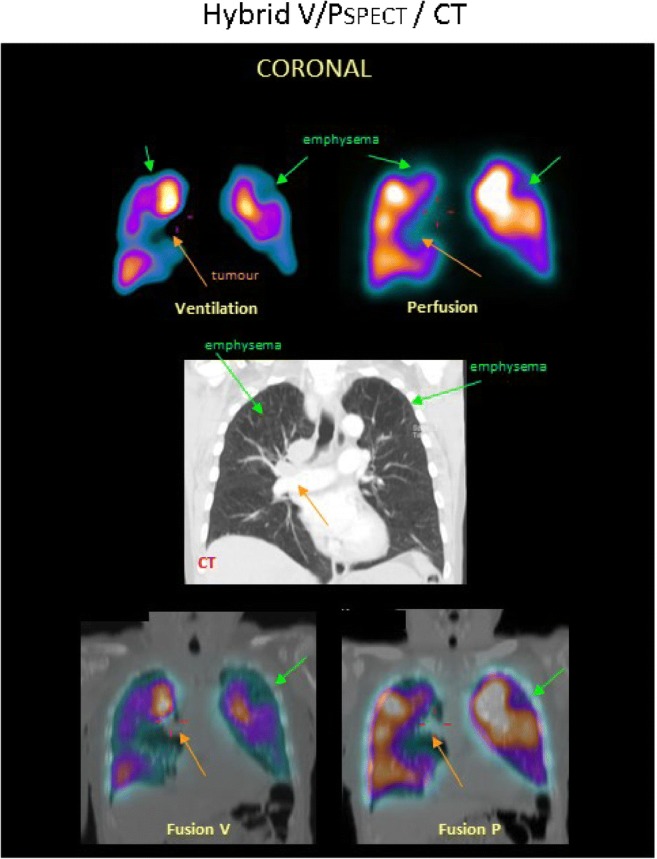
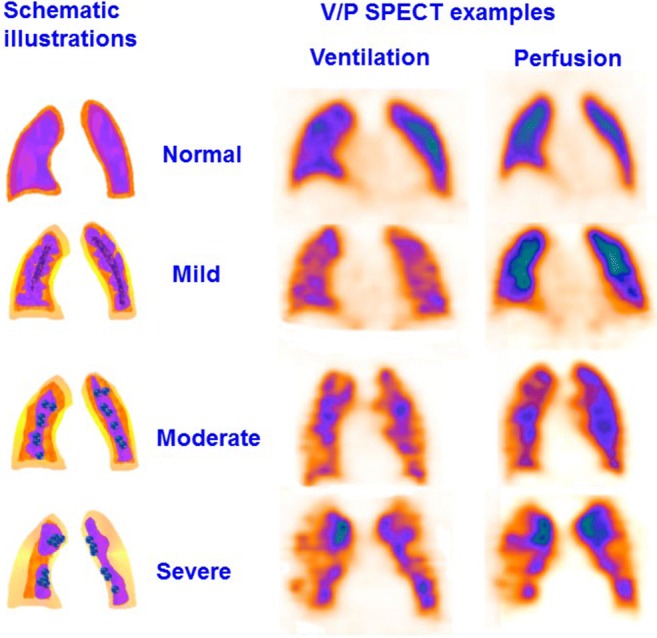
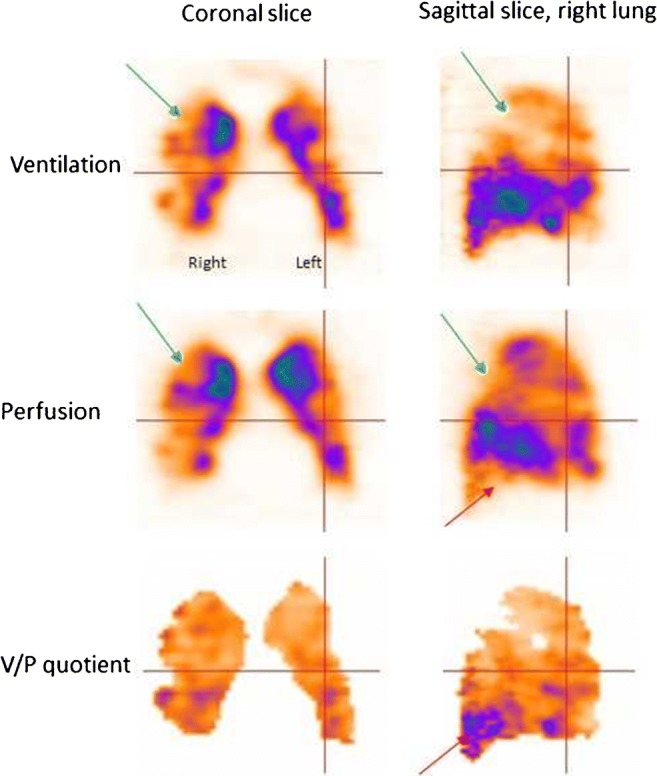
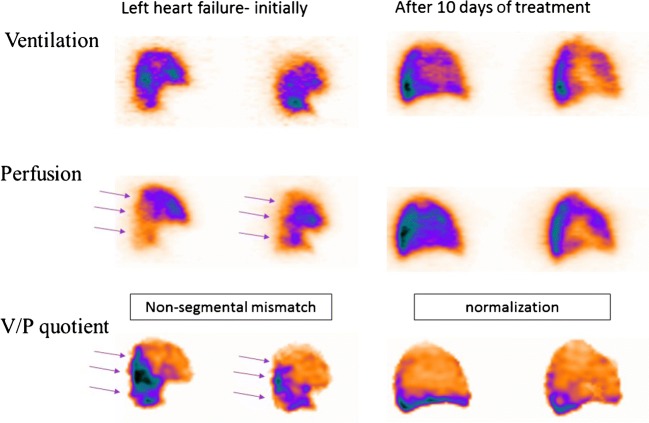
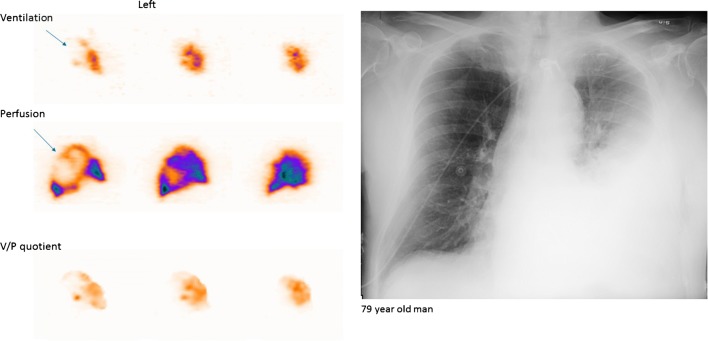
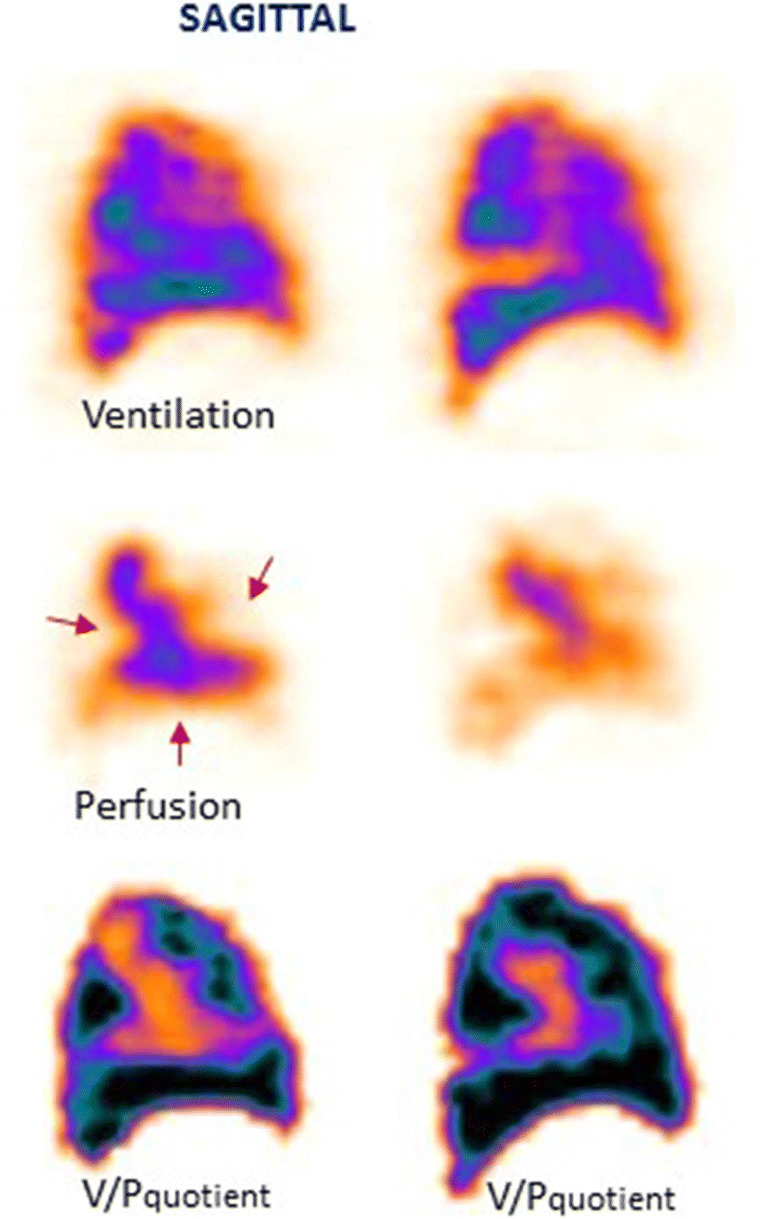
These guidelines update the previous EANM 2009 guidelines on the diagnosis of pulmonary embolism (PE). Relevant new aspects are related to (a) quantification of PE and other ventilation/perfusion defects; (b) follow-up of patients with PE; (c) chronic PE; and (d) description of additional pulmonary physiological changes leading to diagnoses of left ventricular heart failure (HF), chronic obstructive pulmonary disease (COPD) and pneumonia. The diagnosis of PE should be reported when a mismatch of one segment or two subsegments is found. For ventilation, Technegas or krypton gas is preferred over diethylene triamine pentaacetic acid (DTPA) in patients with COPD. Tomographic imaging with V/PSPECT has higher sensitivity and specificity for PE compared with planar imaging. Absence of contraindications makes V/PSPECT an essential method for the diagnosis of PE. When V/PSPECT is combined with a low-dose CT, the specificity of the test can be further improved, especially in patients with other lung diseases. Pitfalls in V/PSPECT interpretation are discussed. In conclusion, V/PSPECT is strongly recommended as it accurately establishes the diagnosis of PE even in the presence of diseases like COPD, HF and pneumonia and has no contraindications.
Keywords: COPD; CTPA; Chronic pulmonary embolism; Left heart failure; Pneumonia; Pulmonary embolism; Pulmonary hypertension; SPECT; V/P SPECT/CT; Ventilation-perfusion.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Comment in
-
Radioaerosols and the updated EANM guideline in ventilation/perfusion imaging.Eur J Nucl Med Mol Imaging. 2020 Jul;47(7):1640-1642. doi: 10.1007/s00259-020-04793-z. Epub 2020 Apr 13. Eur J Nucl Med Mol Imaging. 2020. PMID: 32285154 Free PMC article. No abstract available.
-
Letter to editor.Eur J Nucl Med Mol Imaging. 2020 Jul;47(7):1643-1644. doi: 10.1007/s00259-020-04813-y. Eur J Nucl Med Mol Imaging. 2020. PMID: 32303787 No abstract available.
References
-
- Bajc M, Neilly JB, Miniati M, Schuemichen C, Meignan M, Jonson B. EANM guidelines for ventilation/perfusion scintigraphy: Part 1. Pulmonary imaging with ventilation/perfusion single photon emission tomography. Eur J Nucl Med Mol Imaging. 2009;36:1356–1370. doi: 10.1007/s00259-009-1170-5. - DOI - PubMed
-
- Bajc M, Neilly JB, Miniati M, Schuemichen C, Meignan M, Jonson B. EANM guidelines for ventilation/perfusion scintigraphy: Part 2. Algorithms and clinical considerations for diagnosis of pulmonary emboli with V/P(SPECT) and MDCT. Eur J Nucl Med Mol Imaging. 2009;36:1528–1538. doi: 10.1007/s00259-009-1169-y. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
