

Building Three-Dimensional Intracranial Aneurysm Models from 3D-TOF MRA: a Validation Study
- PMID: 31410678
- PMCID: PMC6841871
- DOI: 10.1007/s10278-019-00256-6
Building Three-Dimensional Intracranial Aneurysm Models from 3D-TOF MRA: a Validation Study
Abstract
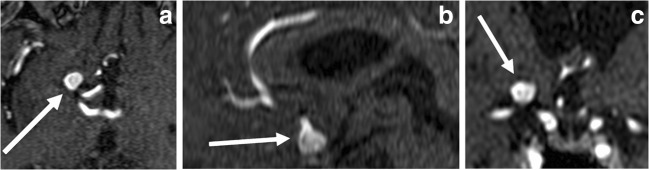
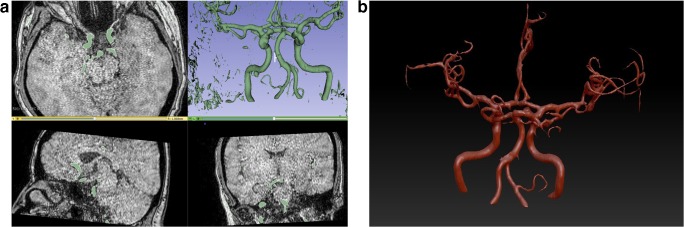
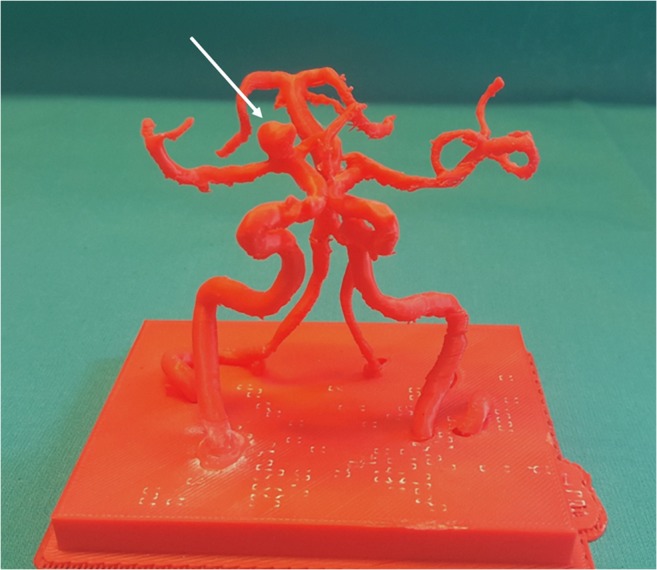
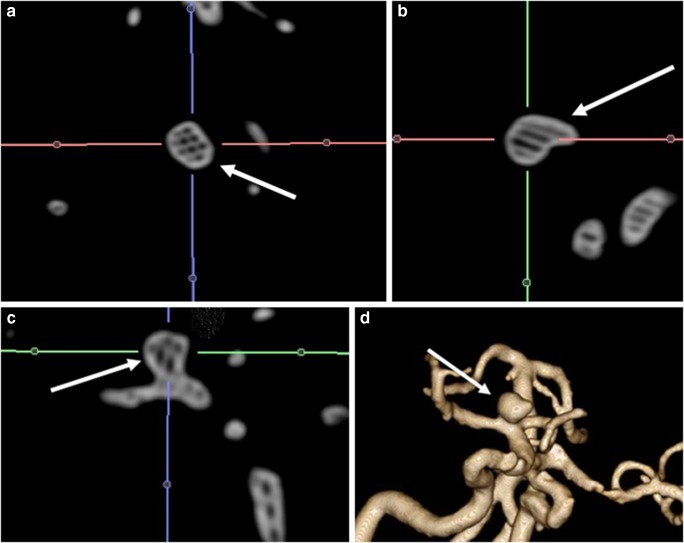
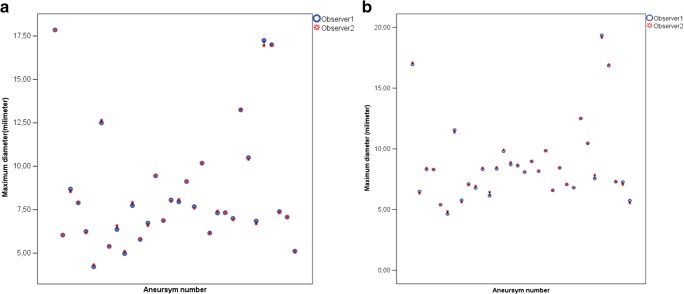
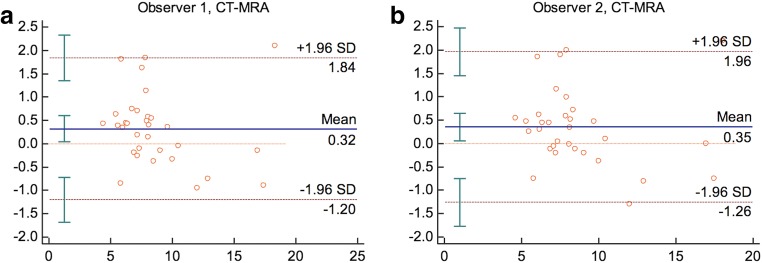
To create realistic three-dimensional (3D) vascular models from 3D time-of-flight magnetic resonance angiography (3D-TOF MRA) of an intracranial aneurysm (IA). Thirty-two IAs in 31 patients were printed using 3D-TOF MRA source images from polylactic acid (PLA) raw material. Two observers measured the maximum IA diameter at the longest width twice separately. A total mean of four measurements as well as each observer's individual average MRA lengths were calculated. After printing, 3D-printed anatomic models (PAM) underwent computed tomography (CT) acquisition and each observer measured them using the same algorithm as applied to MRA. Inter- and intra-observer consistency for the MRA and CT measurements were analyzed using the intraclass correlation coefficient (ICC) and a Bland-Altman plot. The mean maximum aneurysm diameter obtained from four MRA evaluations was 8.49 mm, whereas it was 8.83 mm according to the CT 3D PAM measurement. The Wilcoxon test revealed slightly larger mean CT 3D PAM diameters than the MRA measurements. The Spearman's correlation test yielded a positive correlation between MRA and CT lengths of 3D PAMs. Inter and intra-observer consistency were high in consecutive MRA and CT measurements. According to Bland-Altman analyses, the aneurysmal dimensions obtained from CT were higher for observer 1 and observer 2 (a mean of 0.32 mm and 0.35 mm, respectively) compared to the MRA measurements. CT dimensions were slightly overestimated compared to MRA measurements of the created models. We believe the discrepancy may be related to the Laplacian algorithm applied for surface smoothing and the high slice thickness selection that was used. However, ICC provided high consistency and reproducibility in our cohort. Therefore, it is technically possible to produce 3D intracranial aneurysm models from 3D-TOF MRA images.
Keywords: 3D-TOF magnetic resonance angiography; Intracranial aneurysm; Three-dimensional printing.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- AHA aneurysms description. What you should know about cerebral aneurysms. Cited April 2018. Available from: https://www.strokeassociation.org/en/about-stroke/types-of-stroke/hemorr...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
