

Outcomes of Laparoscopic Liver Resection for Patients with Multiple Hepatocellular Carcinomas Meeting the Milan Criteria: A Propensity Score-Matched Analysis
- PMID: 31411541
- PMCID: PMC6743089
- DOI: 10.1089/lap.2019.0362
Outcomes of Laparoscopic Liver Resection for Patients with Multiple Hepatocellular Carcinomas Meeting the Milan Criteria: A Propensity Score-Matched Analysis
Abstract
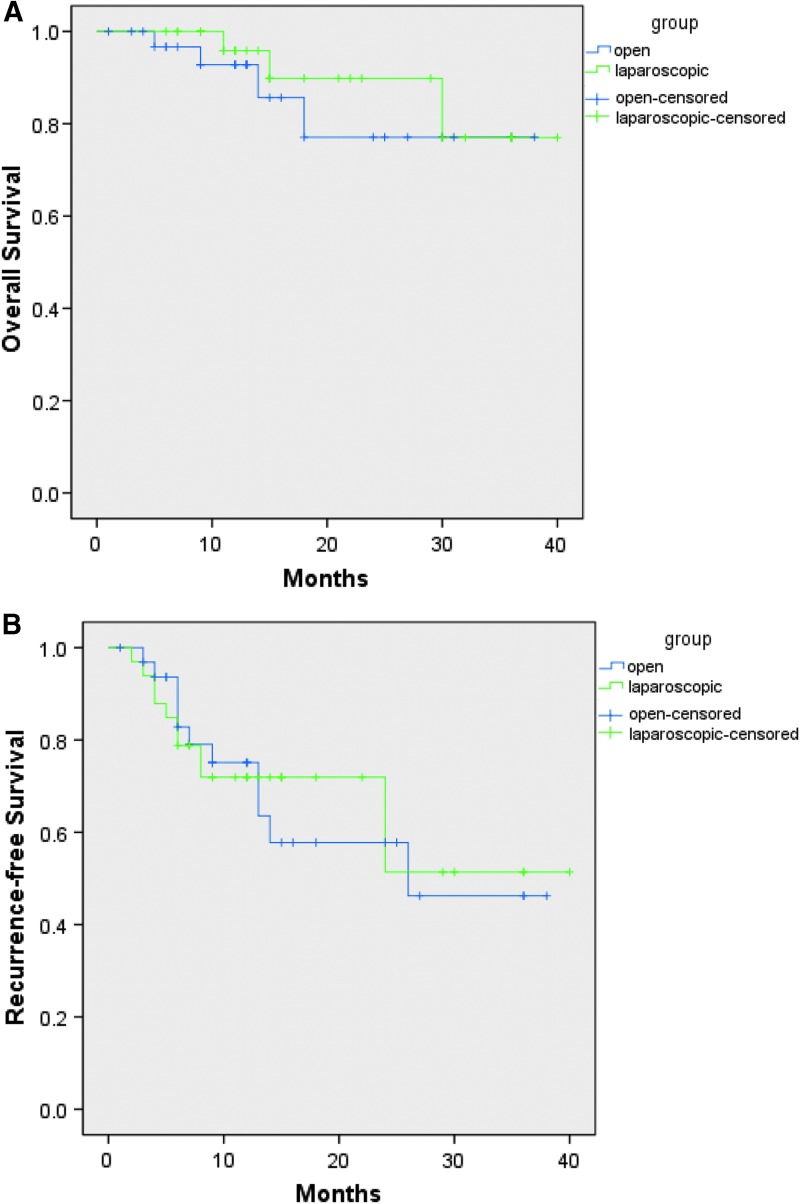
Background: Until now, there is little knowledge about the value of laparoscopic liver resection (LLR) for patients with multiple hepatocellular carcinomas (HCC). This study was performed to assess the efficacy and outcomes of LLR versus open liver resection (OLR) for patients with multiple HCC meeting the Milan criteria. Methods: One hundred fifteen patients with multiple HCC meeting the Milan criteria who underwent liver resection from April 2015 to March 2018 were enrolled into this study. According to the different surgical procedures, patients were divided into LLR group and OLR group. Perioperative and oncological outcomes were compared between the two groups after propensity score matching (PSM) with 1:1 match. Results: Thirty three patients were included into each group after PSM with well-balanced basic level. The intraoperative blood loss in LLR group was less than OLR group before PSM (median, 200 vs. 300 mL, P = .004), but the difference was not statistically significant after PSM (median, 200 vs. 300 mL, P = .064). LLR group showed shorter postoperative hospital stay when compared with OLR group (median, 7 vs. 8 days, respectively, P = .014). The perioperative complications and early mortality were comparable in both groups. There were no significant differences in the term of overall survival (OS. P = .502) or recurrence-free survival (RFS. P = .887) between the two groups after PSM. Conclusions: LLR could be safely and feasibly performed for patients with multiple HCC meeting the Milan criteria in selected patients. It does not increase the risks of postoperative complications and has a similar oncological outcomes compared to OLR.
Keywords: Milan criteria; complications; laparoscopic liver resection; multiple hepatocellular carcinomas; survival rate.
Conflict of interest statement
No competing financial interests exist.
Figures
Similar articles
-
Laparoscopic versus open limited liver resection for hepatocellular carcinoma with liver cirrhosis: a propensity score matching study with the Hiroshima Surgical study group of Clinical Oncology (HiSCO).Surg Endosc. 2020 Nov;34(11):5055-5061. doi: 10.1007/s00464-019-07302-y. Epub 2019 Dec 11. Surg Endosc. 2020. PMID: 31828498
-
Laparoscopic versus open liver resection for hepatocellular carcinoma in elderly patients: a multi-centre propensity score-based analysis.Surg Endosc. 2020 Feb;34(2):658-666. doi: 10.1007/s00464-019-06812-z. Epub 2019 May 15. Surg Endosc. 2020. PMID: 31093748
-
Minor laparoscopic liver resection for Hepatocellular Carcinoma is safer than minor open resection, especially for less compensated cirrhotic patients: Propensity score analysis.Surg Oncol. 2018 Dec;27(4):722-729. doi: 10.1016/j.suronc.2018.10.001. Epub 2018 Oct 3. Surg Oncol. 2018. PMID: 30449499
-
Laparoscopic versus open liver resection for hepatocellular carcinoma in elderly patients: Systematic review and meta-analysis of propensity-score matched studies.Int J Surg. 2022 Sep;105:106821. doi: 10.1016/j.ijsu.2022.106821. Epub 2022 Aug 7. Int J Surg. 2022. PMID: 35948187
-
Association of Laparoscopic Surgery with Improved Perioperative and Survival Outcomes in Patients with Resectable Intrahepatic Cholangiocarcinoma: A Systematic Review and Meta-Analysis from Propensity-Score Matched Studies.Ann Surg Oncol. 2023 Aug;30(8):4888-4901. doi: 10.1245/s10434-023-13498-0. Epub 2023 Apr 28. Ann Surg Oncol. 2023. PMID: 37115372 Free PMC article.
Cited by
-
Survival analysis between laparoscopic and open hepatectomy for hepatocellular carcinoma: a meta-analysis based on reconstructed time-to-event data.Hepatol Int. 2021 Oct;15(5):1215-1235. doi: 10.1007/s12072-021-10219-1. Epub 2021 Jul 13. Hepatol Int. 2021. PMID: 34258665
-
Selecting the Best Approach for the Treatment of Multiple Non-Metastatic Hepatocellular Carcinoma.Cancers (Basel). 2022 Dec 5;14(23):5997. doi: 10.3390/cancers14235997. Cancers (Basel). 2022. PMID: 36497478 Free PMC article. Review.
-
Comparison of survival and post-operation outcomes for minimally invasive versus open hepatectomy in hepatocellular carcinoma: A systematic review and meta-analysis of case-matched studies.Front Oncol. 2022 Oct 20;12:1021804. doi: 10.3389/fonc.2022.1021804. eCollection 2022. Front Oncol. 2022. PMID: 36338679 Free PMC article.
-
Economic analysis of open versus laparoscopic versus robotic hepatectomy: a systematic review and meta-analysis.Eur J Health Econ. 2021 Jun;22(4):585-604. doi: 10.1007/s10198-021-01277-1. Epub 2021 Mar 19. Eur J Health Econ. 2021. PMID: 33740153
-
Leaping the Boundaries in Laparoscopic Liver Surgery for Hepatocellular Carcinoma.Cancers (Basel). 2022 Apr 15;14(8):2012. doi: 10.3390/cancers14082012. Cancers (Basel). 2022. PMID: 35454921 Free PMC article. Review.
References
-
- Lim KC, Chow PKH, Allen JC, Siddiqui FJ, Chan ESY, Tan SB. Systematic review of outcomes of liver resection for early hepatocellular carcinoma within the Milan criteria. Br J Surg 2012;99:1622–1629 - PubMed
-
- Jiang L, Yan L, Wen T, et al. . Comparison of Outcomes of Hepatic Resection and Radiofrequency Ablation for Hepatocellular Carcinoma Patients with Multifocal Tumors Meeting the Barcelona-Clinic Liver Cancer Stage A Classification. J Am Coll Surg 2015;221:951–961 - PubMed
-
- Kim H, Ahn SW, Hong SK, et al. . Survival benefit of liver resection for Barcelona Clinic Liver Cancer stage B hepatocellular carcinoma. Br J Surg 2017;104:1045–1052 - PubMed
-
- Yin L, Li H, Li AJ, et al. . Partial hepatectomy vs. transcatheter arterial chemoembolization for resectable multiple hepatocellular carcinoma beyond Milan Criteria: A RCT. J Hepatol 2014;61:82–88 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous