

Association Between Pancreatic Fistula and Long-term Survival in the Era of Neoadjuvant Chemotherapy
- PMID: 31411659
- PMCID: PMC6694396
- DOI: 10.1001/jamasurg.2019.2272
Association Between Pancreatic Fistula and Long-term Survival in the Era of Neoadjuvant Chemotherapy
Abstract
Importance: In the past decade, the use of neoadjuvant therapy (NAT) has increased for patients with borderline and locally advanced pancreatic ductal adenocarcinoma (PDAC). Data on pancreatic fistula and related overall survival (OS) in this setting are limited.
Objective: To compare postoperative complications in patients undergoing either upfront resection or pancreatectomy following NAT, focusing on clinically relevant postoperative pancreatic fistula (CR-POPF) and potential associations with OS.
Design, setting, and participants: This retrospective cohort study was conducted on data from patients who underwent pancreatic resection for PDAC at the Massachusetts General Hospital from January 1, 2007, to December 31, 2017.
Exposures: Pancreatic cancer surgery with or without NAT.
Main outcomes and measures: Overall morbidity and CR-POPF rates were compared between NAT and upfront resection. Factors associated with CR-POPF were assessed with univariate and multivariate analysis. Survival data were analyzed by Kaplan-Meier curves and a Cox proportional hazards regression model.
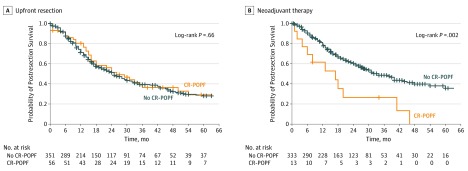
Results: Of 753 patients, 364 were men (48.3%); median (interquartile range) age was 68 (61-75) years. A total of 346 patients (45.9%) received NAT and 407 patients (54.1%) underwent upfront resection. At pathologic examination, NAT was associated with smaller tumor size (mean [SD], 26.0 [15.3] mm vs 32.7 [14.4] mm; P < .001), reduced nodal involvement (102 [25.1%] vs 191 [55.2%]; P < .001), and higher R0 rates (257 [74.3%] vs 239 [58.7%]; P < .001). There were no significant differences in severe complication rate or 90-day mortality. The rate of CR-POPF was 3.6-fold lower in patients receiving NAT vs upfront resection (13 [3.8%] vs 56 [13.8%]; P < .001). In addition, factors associated with CR-POPF changed after NAT, and only soft pancreatic texture was associated with a higher risk of CR-POPF (38.5% vs 6.3%; P < .001). Survival analysis showed no differences between patients with or without CR-POPF after upfront resection (26 vs 25 months; P = .66), but after NAT, a worse overall survival rate was observed in patients with CR-POPF (17 vs 34 months; P = .002). This association was independent of other established predictors of overall survival by multivariate analysis (hazard ratio, 2.80; 95% CI, 1.44-5.45; P < .002).
Conclusions and relevance: Neoadjuvant therapy may be associated with a significant reduction in the rate of CR-POPF. In addition, standard factors associated with CR-POPF appear to be no longer applicable following NAT. However, once CR-POPF occurs, it is associated with a significant reduction in long-term survival. Patients with CR-POPF may require closer follow-up and could benefit from additional therapy.
Conflict of interest statement
Figures
Comment in
-
Prognostic Value of Pancreatic Fistula in Resected Patients With Pancreatic Cancer With Neoadjuvant Therapy.JAMA Surg. 2020 Mar 1;155(3):267-268. doi: 10.1001/jamasurg.2019.5089. JAMA Surg. 2020. PMID: 31877204 No abstract available.
-
Prognostic Value of Pancreatic Fistula in Resected Patients With Pancreatic Cancer With Neoadjuvant Therapy.JAMA Surg. 2020 Mar 1;155(3):268-269. doi: 10.1001/jamasurg.2019.5090. JAMA Surg. 2020. PMID: 31877212 No abstract available.
-
Prognostic Value of Pancreatic Fistula in Resected Patients With Pancreatic Cancer With Neoadjuvant Therapy-Reply.JAMA Surg. 2020 Mar 1;155(3):269. doi: 10.1001/jamasurg.2019.5091. JAMA Surg. 2020. PMID: 32186694 No abstract available.
References
-
- Michelakos T, Pergolini I, Fernández-del Castillo C, et al. . Predictors of resectability and survival in patients with borderline and locally advanced pancreatic cancer who underwent neoadjuvant treatment with FOLFIRINOX. Ann Surg. 2019;269(4):733-740. doi:10.1097/SLA.0000000000002600 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
