

Value of Partial Nephrectomy for Renal Cortical Tumors of cT2 or Greater Stage: A Risk-benefit Analysis of Renal Function Preservation Versus Increased Postoperative Morbidity
- PMID: 31411969
- PMCID: PMC8407532
- DOI: 10.1016/j.euo.2019.04.003
Value of Partial Nephrectomy for Renal Cortical Tumors of cT2 or Greater Stage: A Risk-benefit Analysis of Renal Function Preservation Versus Increased Postoperative Morbidity
Abstract
Background: Indications for partial nephrectomy (PN) have expanded to include larger tumors. Compared with radical nephrectomy (RN), PN reduces the risk of chronic kidney disease but is associated with higher morbidity.
Objective: To explore whether the benefit of PN (preservation of estimated glomerular filtration rate [eGFR] ≥60ml/min/1.73m2 1yr postoperatively) over RN is offset by higher morbidity for cT2-cT3a tumors.
Design, setting, and participants: A total of 1921 patients with renal cortical tumors who underwent nephrectomy between 2000 and 2012 were analyzed, with 297 having clinical stage T2 or higher disease.
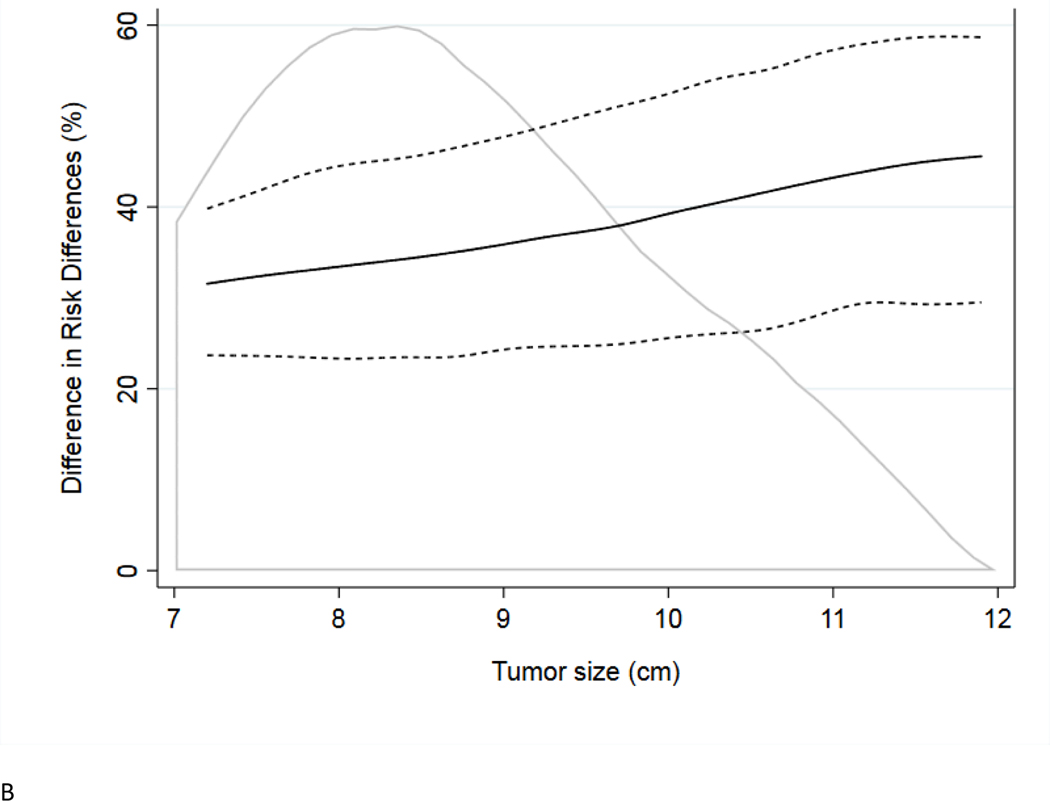
Outcome measurements and statistical analysis: Multivariable logistic regression models adjusted for age, tumor size, and comorbidities were used to calculate the risk of complications within 90d and the risk of low eGFR across a range of tumor sizes. Models were created separately for RN and PN, and the difference between risk estimates was calculated.
Results and limitations: For tumors with diameters between 7 and 12cm, the risk of eGFR downgrade associated with RN was higher than the risk of complications associated with PN. The magnitude of the risk of eGFR downgrade was similar to the magnitude of complications risk across all tumor sizes. Our analysis was performed at a single institution, and used only tumor size to compare the risk and benefits of surgery.
Conclusions: Our study suggests that PN is associated with higher eGFR preservation than RN for cT2 or greater renal tumors. The magnitude of this advantage offsets the higher morbidity observed with PN.
Patient summary: When treating a large kidney tumor, it is difficult to decide whether it is better to remove the whole kidney or remove just the tumor. The second option improves postoperative renal function but is more complex. We tried to find whether there is a tumor size at which one technique should be used over the other.
Keywords: Chronic kidney disease; Complications; Nephrectomy; Nephron-sparing surgery; Renal cell carcinoma.
Copyright © 2019 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures



References
-
- Touijer K, Jacqmin D, Kavoussi LR, et al.The expanding role of partial nephrectomy: a critical analysis of indications, results, and complications. Eur Urol 2010;57:214–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
