

Imbalanced Corticospinal and Reticulospinal Contributions to Spasticity in Humans with Spinal Cord Injury
- PMID: 31413076
- PMCID: PMC6774405
- DOI: 10.1523/JNEUROSCI.1106-19.2019
Imbalanced Corticospinal and Reticulospinal Contributions to Spasticity in Humans with Spinal Cord Injury
Abstract
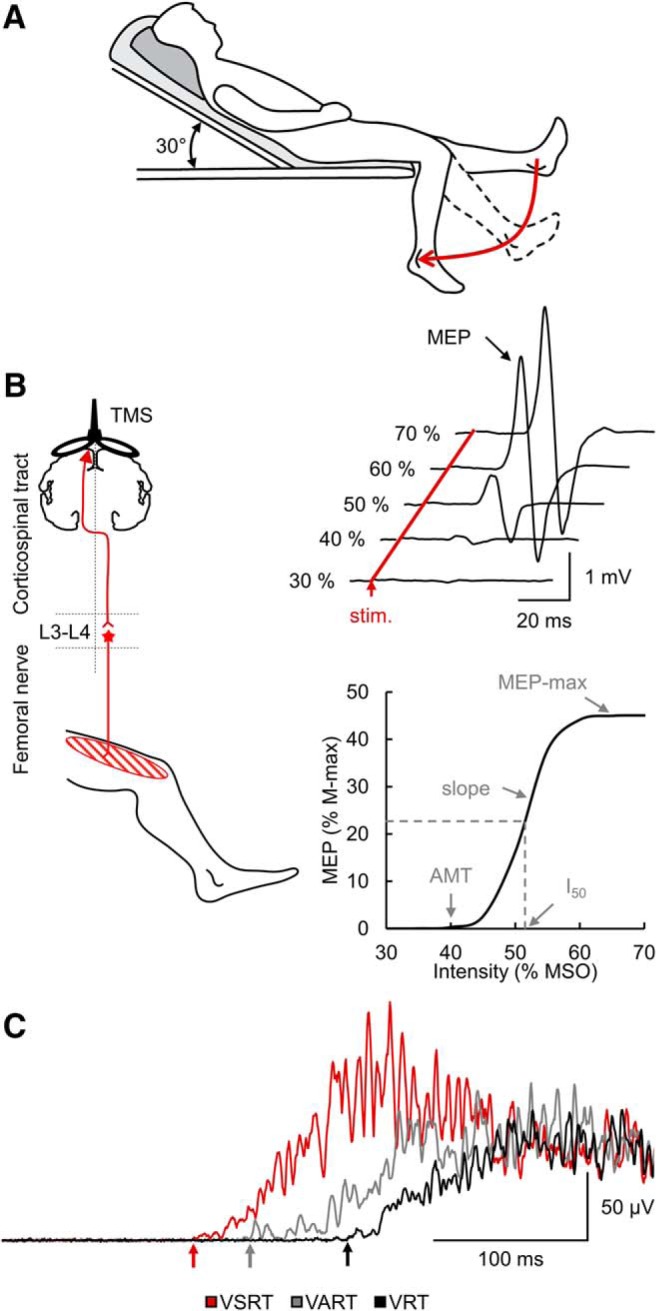
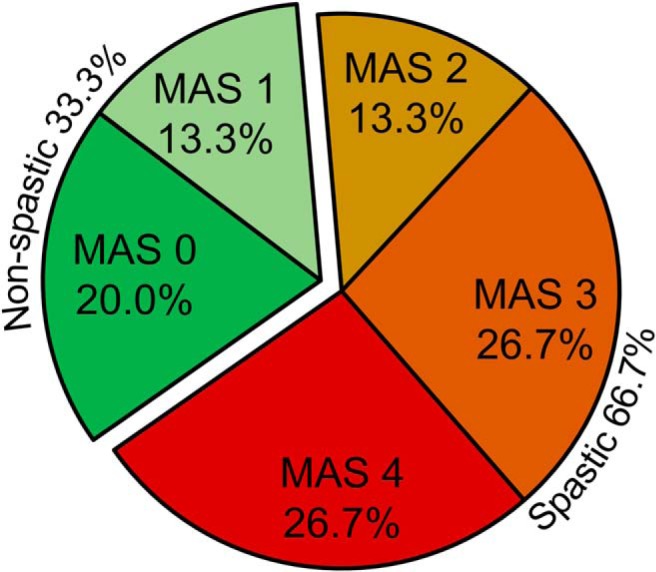
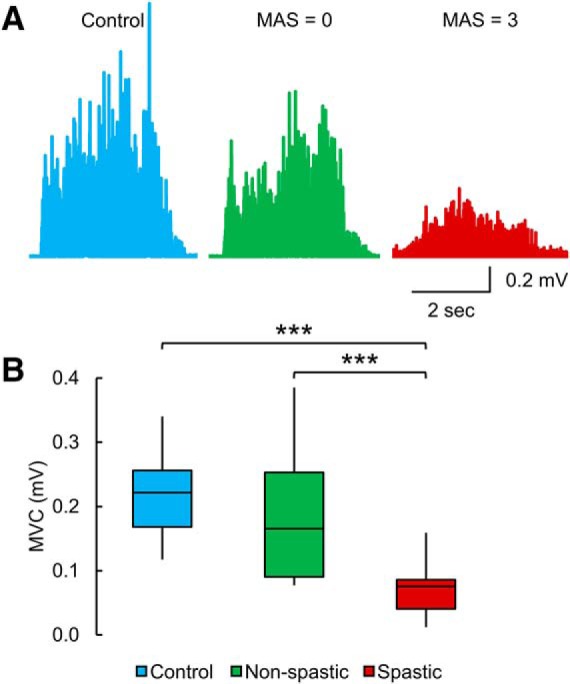
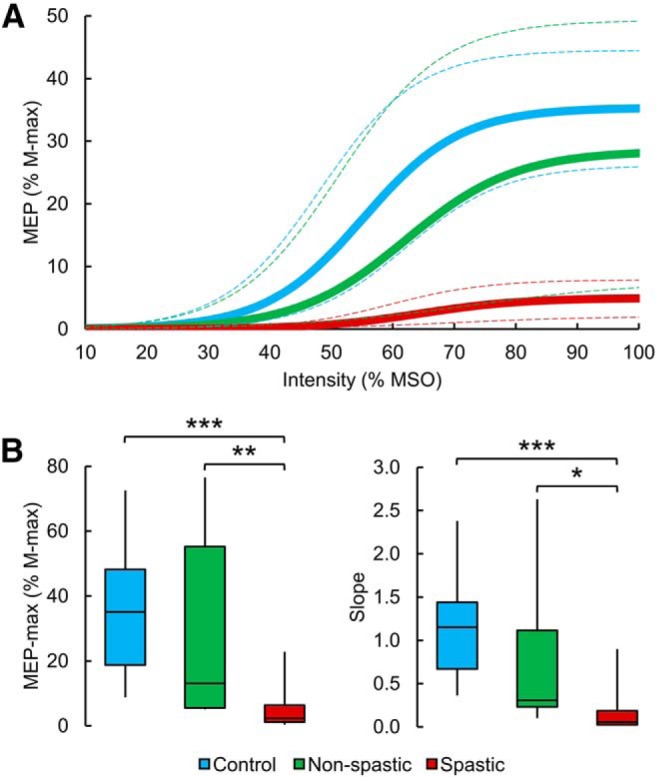
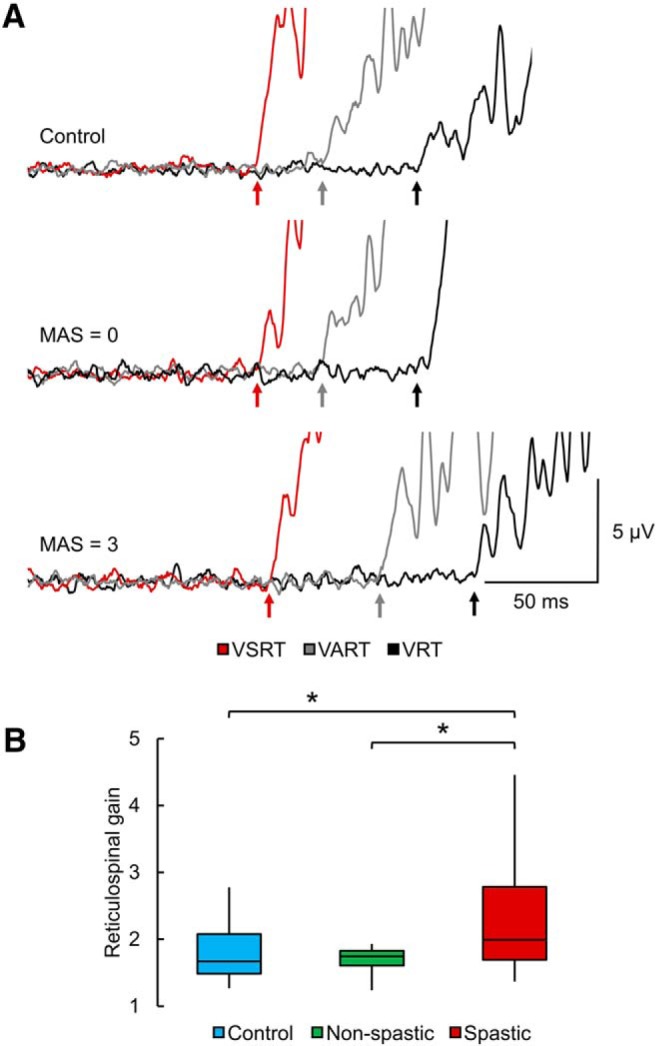
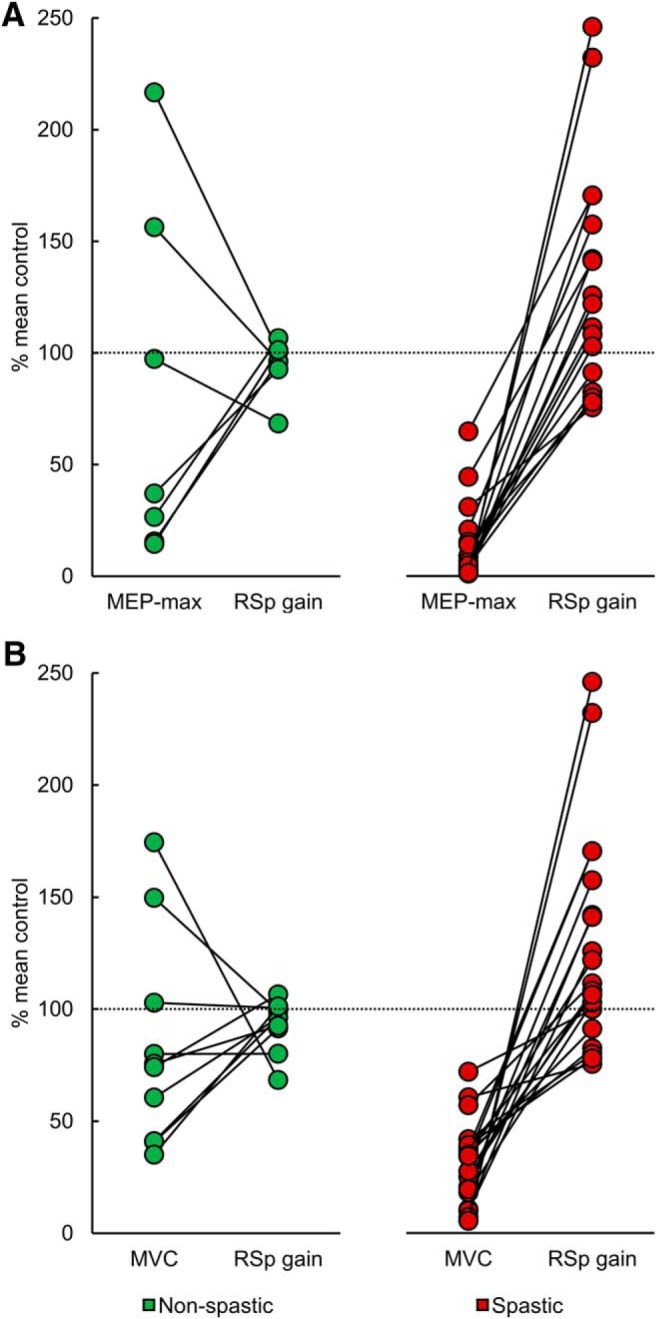
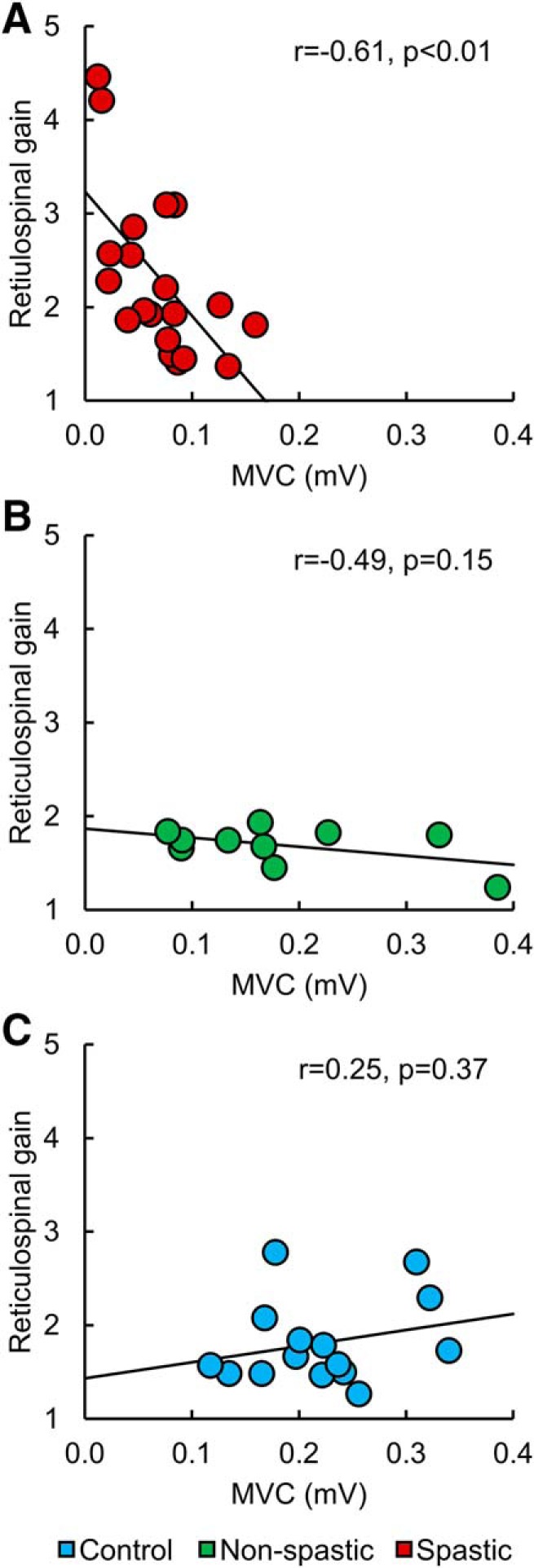
Damage to the corticospinal and reticulospinal tract has been associated with spasticity in humans with upper motor neuron lesions. We hypothesized that these descending motor pathways distinctly contribute to the control of a spastic muscle in humans with incomplete spinal cord injury (SCI). To test this hypothesis, we examined motor-evoked potentials (MEPs) elicited by transcranial magnetic stimulation over the leg representation of the primary motor cortex, maximal voluntary contractions (MVCs), and the StartReact response (shortening in reaction time evoked by a startling stimulus) in the quadriceps femoris muscle in male and females with and without incomplete SCI. A total of 66.7% of the SCI participants showed symptoms of spasticity, whereas the other 33.3% showed no or low levels of spasticity. We found that participants with spasticity had smaller MEPs and MVCs and larger StartReact compared with participants with no or low spasticity and control subjects. These results were consistently present in spastic subjects but not in the other populations. Clinical scores of spasticity were negatively correlated with MEP-max and MVC values and positively correlated with shortening in reaction time. These findings provide evidence for lesser corticospinal and larger reticulospinal influences to spastic muscles in humans with SCI and suggest that these imbalanced contributions are important for motor recovery.SIGNIFICANCE STATEMENT Although spasticity is one of the most common symptoms manifested in humans with spinal cord injury (SCI) to date, its mechanisms of action remain poorly understood. We provide evidence, for the first time, of imbalanced contributions of the corticospinal and reticulospinal tract to control a spastic muscle in humans with chronic incomplete SCI. We found that participants with SCI with spasticity showed small corticospinal responses and maximal voluntary contractions and larger reticulospinal gain compared with participants with no or low spasticity and control subjects. These results were consistently present in spastic subjects but not in the other populations. We showed that imbalanced corticospinal and reticulospinal tract contributions are more pronounced in participants with chronic incomplete SCI with lesser recovery.
Keywords: corticospinal pathway; muscle weakness; reticulospinal pathway; spasticity; voluntary drive.
Copyright © 2019 the authors.
Figures
References
-
- Asboth L, Friedli L, Beauparlant J, Martinez-Gonzalez C, Anil S, Rey E, Baud L, Pidpruzhnykova G, Anderson MA, Shkorbatova P, Batti L, Pagès S, Kreider J, Schneider BL, Barraud Q, Courtine G (2018) Cortico-reticulo-spinal circuit reorganization enables functional recovery after severe spinal cord contusion. Nat Neurosci 21:576–588. 10.1038/s41593-018-0093-5 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical