

Regulatable interleukin-12 gene therapy in patients with recurrent high-grade glioma: Results of a phase 1 trial
- PMID: 31413142
- PMCID: PMC7286430
- DOI: 10.1126/scitranslmed.aaw5680
Regulatable interleukin-12 gene therapy in patients with recurrent high-grade glioma: Results of a phase 1 trial
Abstract
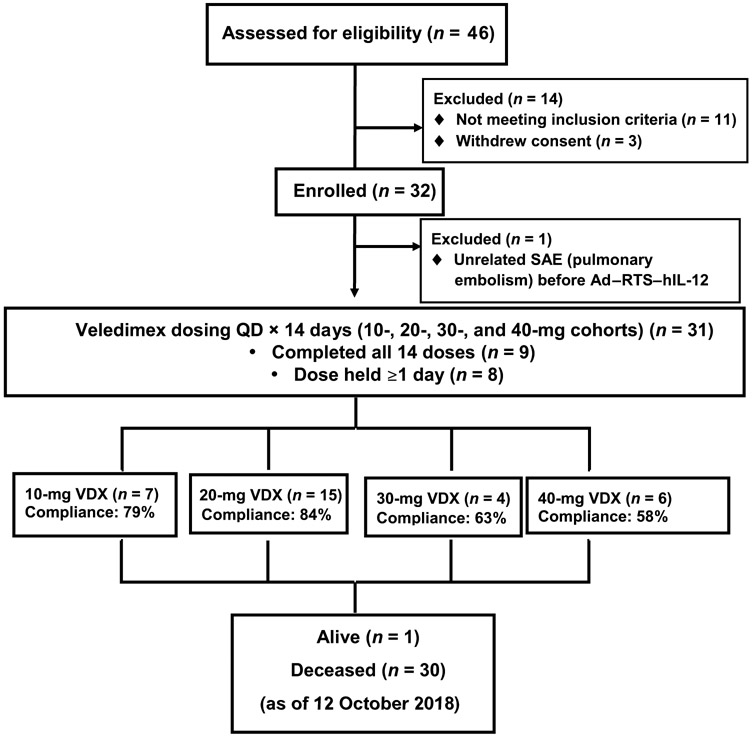
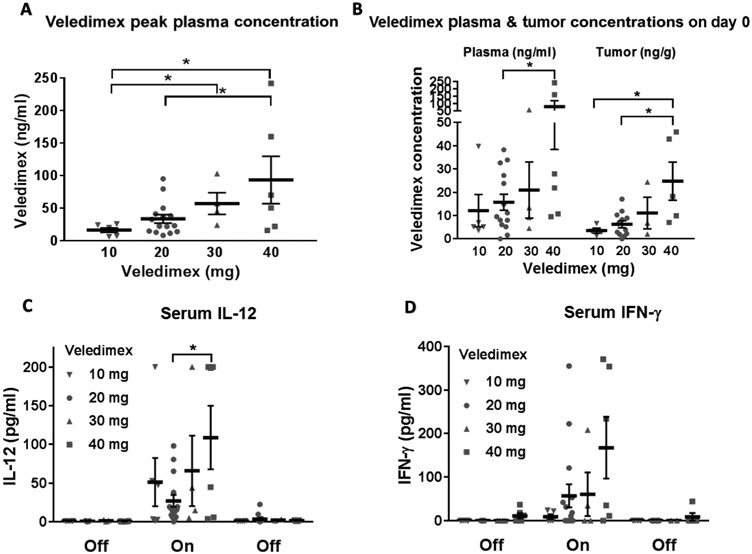
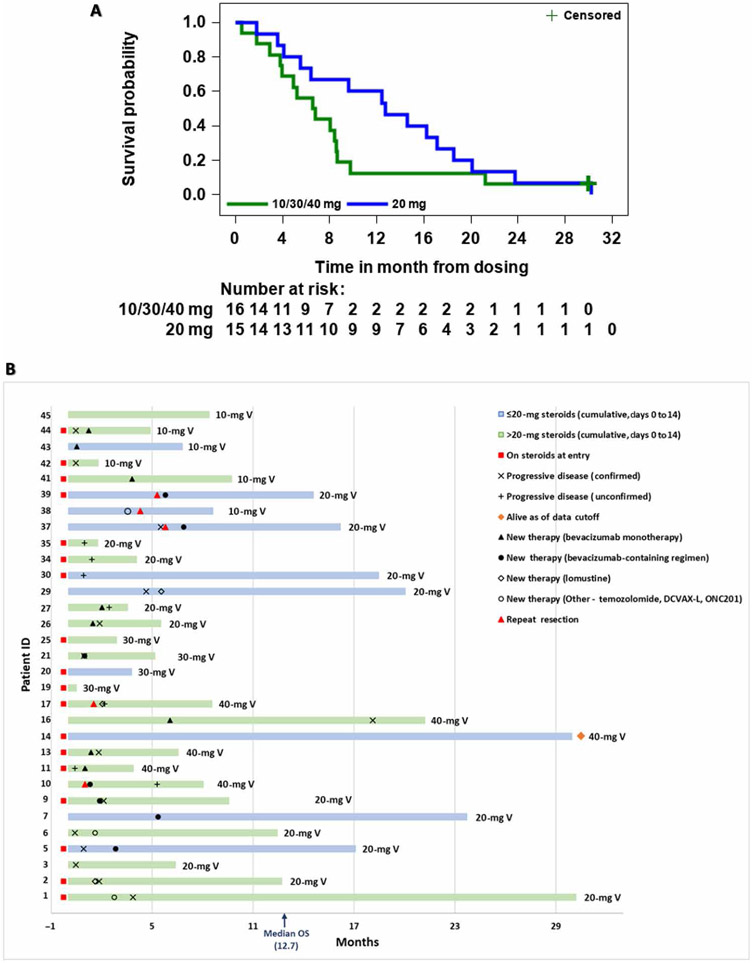
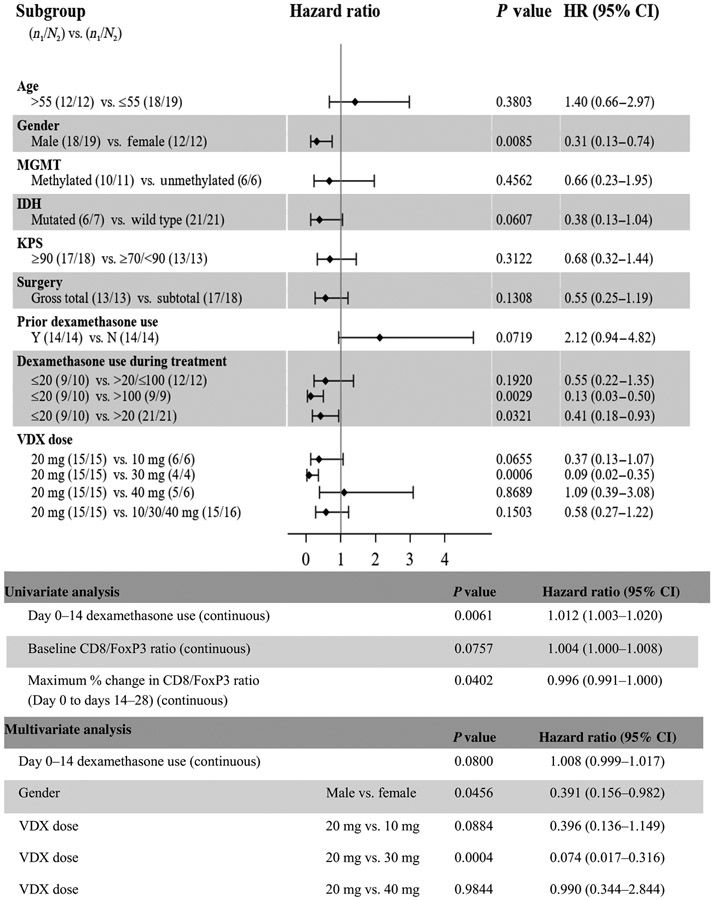
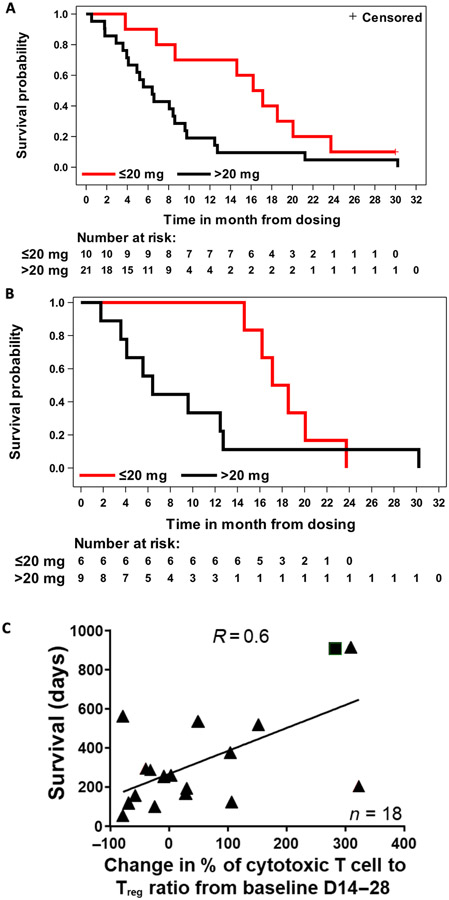
Human interleukin-12 (hIL-12) is a cytokine with anticancer activity, but its systemic application is limited by toxic inflammatory responses. We assessed the safety and biological effects of an hIL-12 gene, transcriptionally regulated by an oral activator. A multicenter phase 1 dose-escalation trial (NCT02026271) treated 31 patients undergoing resection of recurrent high-grade glioma. Resection cavity walls were injected (day 0) with a fixed dose of the hIL-12 vector (Ad-RTS-hIL-12). The oral activator for hIL-12, veledimex (VDX), was administered preoperatively (assaying blood-brain barrier penetration) and postoperatively (measuring hIL-12 transcriptional regulation). Cohorts received 10 to 40 mg of VDX before and after Ad-RTS-hIL-12. Dose-related increases in VDX, IL-12, and interferon-γ (IFN-γ) were observed in peripheral blood, with about 40% VDX tumor penetration. Frequency and severity of adverse events, including cytokine release syndrome, correlated with VDX dose, reversing promptly upon discontinuation. VDX (20 mg) had superior drug compliance and 12.7 months median overall survival (mOS) at mean follow-up of 13.1 months. Concurrent corticosteroids negatively affected survival: In patients cumulatively receiving >20 mg versus ≤20 mg of dexamethasone (days 0 to 14), mOS was 6.4 and 16.7 months, respectively, in all patients and 6.4 and 17.8 months, respectively, in the 20-mg VDX cohort. Re-resection in five of five patients with suspected recurrence after Ad-RTS-hIL-12 revealed mostly pseudoprogression with increased tumor-infiltrating lymphocytes producing IFN-γ and programmed cell death protein 1 (PD-1). These inflammatory infiltrates support an immunological antitumor effect of hIL-12. This phase 1 trial showed acceptable tolerability of regulated hIL-12 with encouraging preliminary results.
Copyright © 2019 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures

References
-
- Mrugala MM, Advances and challenges in the treatment of glioblastoma: A clinician’s perspective. Discov. Med 15, 221–230 (2013). - PubMed
-
- Reardon DA, Wen PY, Wucherpfennig KW, Sampson JH, Immunomodulation for glioblastoma. Curr. Opin. Neurol 30, 361–369 (2017). - PubMed
-
- Ricklefs FL, Alayo Q, Krenzlin H, Mahmoud AB, Speranza MC, Nakashima H, Hayes JL, Lee K, Balaj L, Passaro C, Rooj AK, Krasemann S, Carter BS, Chen CC, Steed T, Treiber J, Rodig S, Yang K, Nakano I, Lee H, Weissleder R, Breakefield XO, Godlewski J, Westphal M, Lamszus K, Freeman GJ, Bronisz A, Lawler SE, Chiocca EA, Immune evasion mediated by PD-L1 on glioblastoma-derived extracellular vesicles. Sci. Adv 4, eaar2766 (2018). - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
