

Prognostic implications of left ventricular strain by speckle-tracking echocardiography in the general population: a meta-analysis
- PMID: 31413582
- PMCID: PMC6661977
- DOI: 10.2147/VHRM.S206747
Prognostic implications of left ventricular strain by speckle-tracking echocardiography in the general population: a meta-analysis
Abstract
Purpose: Left ventricular (LV) mechanics by speckle-tracking echocardiography (STE) is prognostic in patients with cardiovascular diseases, but evidence related to community-dwelling individuals is uncertain. We therefore performed a systematic review and meta-analysis of STE as a predictor of adverse outcomes in the general population.
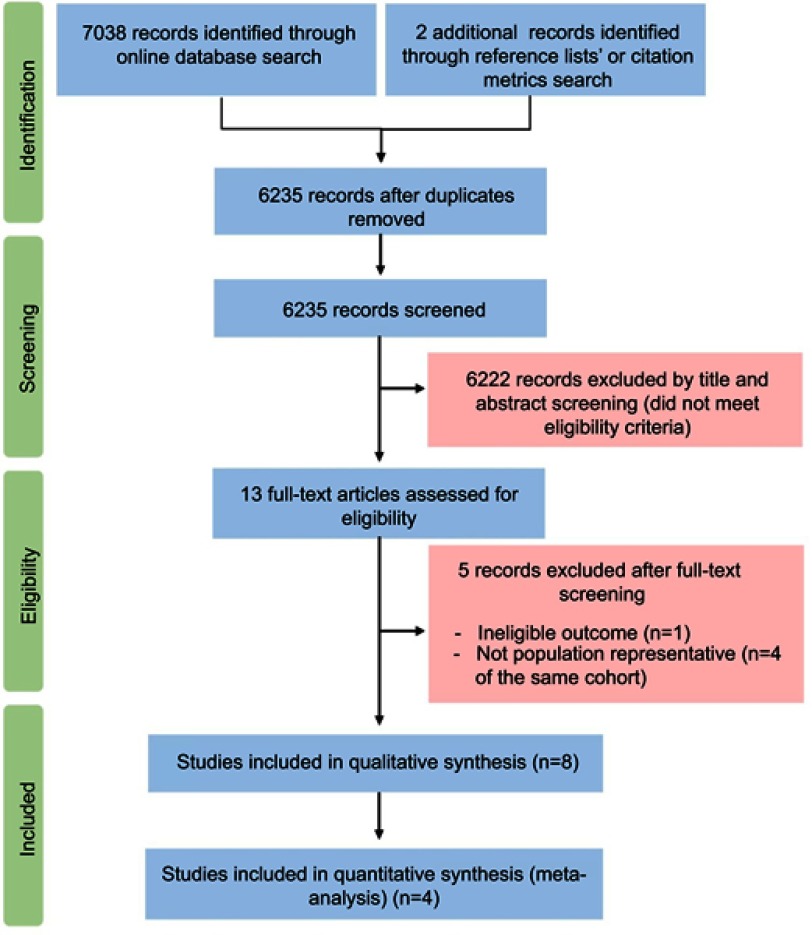
Methods: PRISMA guidelines were followed and MEDLINE and EMBASE were searched to identify eligible studies. Primary outcome was all-cause mortality and secondary outcomes were composite cardiac and cardiovascular end-point. Random effects meta-analysis was performed, and a modified Newcastle-Ottawa Assessment Scale was used for quality assessment.
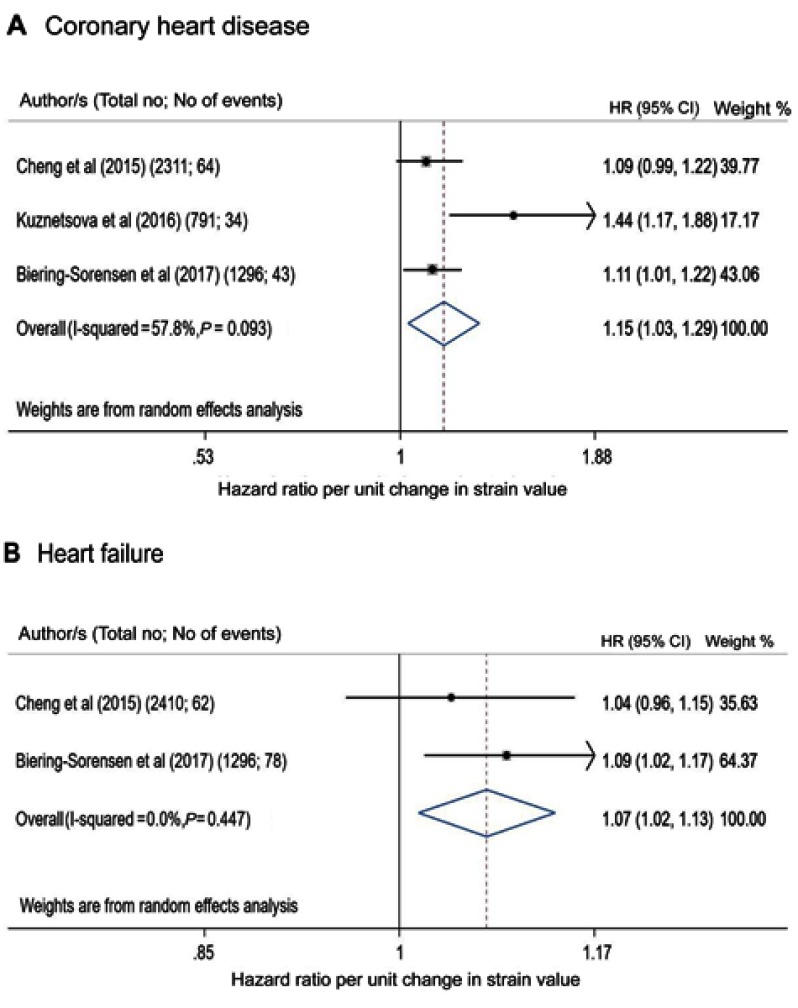
Results: Eight papers matched the predefined criteria (total number of individuals studied=11,744). All publications assessed global longitudinal strain (GLS) by two-dimensional speckle-tracking echocardiography (2D-STE), one assessed circumferential, radial and transverse strains, and one assessed GLS-derived post-systolic shortening. None assessed LV rotational measures in association with outcomes. Two studies reported associations between GLS and all-cause mortality and composite cardiovascular end-point. Six papers reported an association between GLS and composite cardiac end-point, three of which were from the same study. Four papers were suitable for meta-analysis. GLS predicted all-cause mortality (pooled minimally adjusted HR per unit strain (%)=1.07 [95% CI 1.03-1.11], p=0.001), and composite cardiovascular (pooled maximally adjusted HR=1.18 [1.09-1.28], p<0.0001) and cardiac (HR=1.08 [1.02-1.14], p=0.006) end-points. GLS also predicted coronary heart disease (HR=1.15 [1.03-1.29], p=0.017) and heart failure (HR=1.07 [1.02-1.13], p=0.012). The quality of all studies was good.
Conclusions: This study provides some evidence that STE may have utility as a measure of cardiac function and risk in the general population. 2D-STE-based GLS predicts total mortality, major adverse cardiac and cardiovascular end-points in community-dwelling individuals in a limited number of studies. Despite this, this systematic review also highlights important knowledge gaps in the current literature and further evidence is needed regarding the prognostic value of LV mechanics in unselected older populations.Registration number: CRD42018090302.
Keywords: cardiovascular disease; community-dwelling individuals; left ventricular strain; mortality.
Conflict of interest statement
This work was presented at the British Society of Echocardiography 2018 as a presentation with interim findings. Professor Alun Hughes reports grants from British Heart Foundation, during the conduct of the study. The authors report no other conflicts of interest in this work.
Figures

Similar articles
-
Prognostic implications of left ventricular strain by speckle-tracking echocardiography in population-based studies: a systematic review protocol of the published literature.BMJ Open. 2018 Jul 16;8(7):e023346. doi: 10.1136/bmjopen-2018-023346. BMJ Open. 2018. PMID: 30012795 Free PMC article.
-
Global Longitudinal Strain by Echocardiography Predicts Long-Term Risk of Cardiovascular Morbidity and Mortality in a Low-Risk General Population: The Copenhagen City Heart Study.Circ Cardiovasc Imaging. 2017 Mar;10(3):e005521. doi: 10.1161/CIRCIMAGING.116.005521. Circ Cardiovasc Imaging. 2017. PMID: 28264868 Free PMC article.
-
Association Between Global Longitudinal Strain and Cardiovascular Events in Patients With Left Bundle Branch Block Assessed Using Two-Dimensional Speckle-Tracking Echocardiography.J Am Soc Echocardiogr. 2018 Jan;31(1):52-63.e6. doi: 10.1016/j.echo.2017.08.016. Epub 2017 Nov 2. J Am Soc Echocardiogr. 2018. PMID: 29079044
-
Echocardiographic assessment of left ventricular mechanics in individuals with mitral valve prolapse: a systematic review and meta-analysis.Int J Cardiovasc Imaging. 2024 Aug;40(8):1617-1629. doi: 10.1007/s10554-024-03179-8. Epub 2024 Jul 8. Int J Cardiovasc Imaging. 2024. PMID: 38976111
-
Echocardiographic parameters of cardiac structure and function in the diagnosis of acute myocarditis in adult patients: A systematic review and meta-analysis.Echocardiography. 2024 Feb;41(2):e15760. doi: 10.1111/echo.15760. Echocardiography. 2024. PMID: 38345413
Cited by
-
Automated analysis of limited echocardiograms: Feasibility and relationship to outcomes in COVID-19.Front Cardiovasc Med. 2022 Jul 22;9:937068. doi: 10.3389/fcvm.2022.937068. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35935624 Free PMC article.
-
Haemodynamic Forces: Emerging Markers of Ventricular Remodelling in Multiple Myeloma Cardiovascular Baseline Risk Assessment.Cancers (Basel). 2024 Sep 4;16(17):3081. doi: 10.3390/cancers16173081. Cancers (Basel). 2024. PMID: 39272939 Free PMC article.
-
Decreased diastolic hydraulic forces incrementally associate with survival beyond conventional measures of diastolic dysfunction.Sci Rep. 2023 Sep 29;13(1):16396. doi: 10.1038/s41598-023-41694-1. Sci Rep. 2023. PMID: 37773251 Free PMC article.
-
Relationship Between Image Quality and Bias in 3D Echocardiographic Measures: Data From the SABRE (Southall and Brent Revisited) Study.J Am Heart Assoc. 2022 May 3;11(9):e019183. doi: 10.1161/JAHA.120.019183. Epub 2022 Apr 27. J Am Heart Assoc. 2022. PMID: 35475343 Free PMC article.
-
Prognostic Significance of Echocardiographic Measures of Cardiac Remodeling in the Community.Curr Cardiol Rep. 2021 Jun 3;23(7):86. doi: 10.1007/s11886-021-01512-4. Curr Cardiol Rep. 2021. PMID: 34081212 Review.
References
-
- Potter E, Marwick TH. Assessment of left ventricular function by echocardiography: the case for routinely adding global longitudinal strain to ejection fraction. JACC Cardiovasc Imaging. 2018;11(2 Pt 1):260–274. - PubMed
-
- Mor-Avi V, Lang RM, Badano LP, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese society of echocardiography. J Am Soc Echocardiogr. 2011;24(3):277–313. doi:10.1016/j.echo.2011.01.015 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
