

Early Predictors of Microsurgical Reconstruction in Brachial Plexus Birth Palsy
- PMID: 31413672
- PMCID: PMC6604547
Early Predictors of Microsurgical Reconstruction in Brachial Plexus Birth Palsy
Abstract
Background: Microsurgical reconstruction is indicated for infants with brachial plexus birth palsy (BPBP) that demonstrate limited spontaneous neurological recovery. This investigation defines the demographic, perinatal, and physical examination characteristics leading to microsurgical reconstruction.
Methods: Infants enrolled in a prospective multicenter investigation of BPBP were evaluated. Microsurgery was performed at the discretion of the treating provider/center. Inclusion required enrollment prior to six months of age and follow-up evaluation beyond twelve months of age. Demographic, perinatal, and examination characteristics were investigated as possible predictors of microsurgical reconstruction. Toronto Test scores and Hospital for Sick Children Active Movement Scale (AMS) scores were used if obtained prior to three months of age. Univariate and multivariate logistic regression analyses were performed.
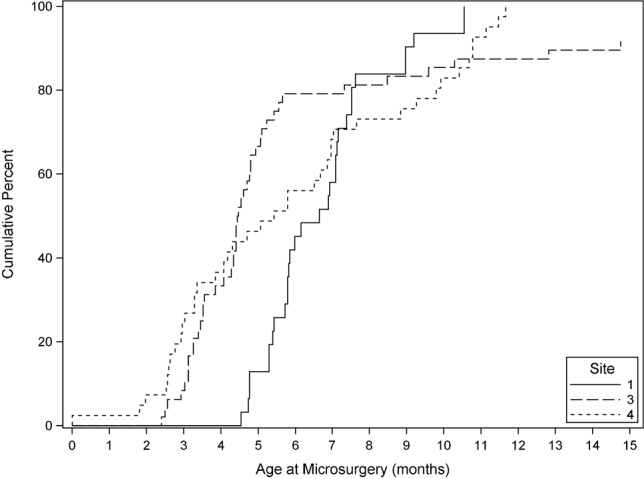
Results: 365 patients from six regional medical centers met the inclusion criteria. 127 of 365 (35%) underwent microsurgery at a median age of 5.4 months, with microsurgery rates and timing varying significantly by site. Univariate analysis demonstrated that several factors were associated with microsurgery including race, gestational diabetes, neonatal asphyxia, neonatal intensive care unit admission, Horner's syndrome, Toronto Test score, and AMS scores for finger/thumb/wrist flexion, finger/thumb extension, wrist extension, elbow flexion, and elbow extension. In multivariate analysis, four factors independently predicted microsurgical intervention including Horner's syndrome, mean AMS score for finger/thumb/ wrist flexion <4.5, AMS score for wrist extension <4.5, and AMS score for elbow flexion <4.5. In this cohort, microsurgical rates increased as the number of these four factors present increased from zero to four: 0/4 factors = 0%, 1/4 factors = 22%, 2/4 factors = 43%, 3/4 factors = 76%, and 4/4 factors = 93%.
Conclusions: In patients with BPBP, early physical examination findings independently predict microsurgical intervention. These factors can be used to provide counseling in early infancy for families regarding injury severity and plan for potential microsurgical intervention.Level of Evidence: Prognostic Level I.
Keywords: birth; brachial; obstetric; palsy; plexus.
Conflict of interest statement
Disclosures: The authors report no potential conflicts of interest related to this study.
Figures
References
-
- DeFrancesco CJ, Shah DK, Rogers BH, et al. The epidemiology of brachial plexus birth palsy in the United States: declining incidence and evolving risk factors. J Pediatr Orthop. e-published ahead of print. - PubMed
-
- Greenwald AG, Schute PC, Shiveley JL. Brachial plexus birth palsy: a 10-year report on the incidence and prognosis. J Pediatr Orthop. 1984;4(6):689–692. - PubMed
-
- Hardy AE. Birth injuries of the brachial plexus: incidence and prognosis. J Bone Joint Surg Br. 1981;63-B(1):98–101. - PubMed
-
- Hale HB, Bae DS, Waters PM. Current concepts in the management of brachial plexus birth palsy. J Hand Surg Am. 2010;35(2):322–331. - PubMed
-
- Narakas AO. [Injuries of the brachial plexus and neighboring peripheral nerves in vertebral fractures and other trauma of the cervical spine] Orthopade. 1987;16(1):81–86. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous