

40 Years of Change in Age- and Stage-Specific Cancer Incidence Rates in US Women and Men
- PMID: 31414075
- PMCID: PMC6686848
- DOI: 10.1093/jncics/pkz038
40 Years of Change in Age- and Stage-Specific Cancer Incidence Rates in US Women and Men
Abstract
Background: Studies have documented a temporal increase in incidence for several cancers in US young adults aged 25 to 39-years, including noncardia gastric cancer, colorectal cancer, and distant-stage breast cancer. To further characterize trends in young adults, we assessed age-specific and stage-specific incidence trends from 1975 to 2015, overall (all malignant cancers combined), and for 18 and 16 cancer sites in women and men, respectively.
Methods: We used US population-based data from the Surveillance, Epidemiology, and End Results Program to obtain overall and site-specific cancer incidence rates by sex and age group. We individually analyzed cancer sites with an incidence rate of at least 5 per 100 000 in 2015, accounting for greater than 90% of all cancer diagnoses. We estimated annual percent changes (APCs) using segment log-linear regression performed with joinpoint software; multiple permutation testing was used to identify inflection points. We forecasted overall cancer incidence through 2030 using age-period-cohort regression models.
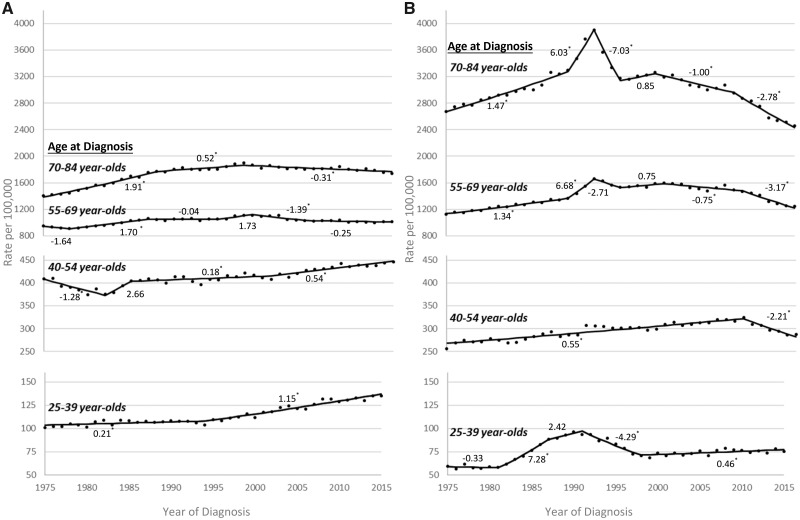
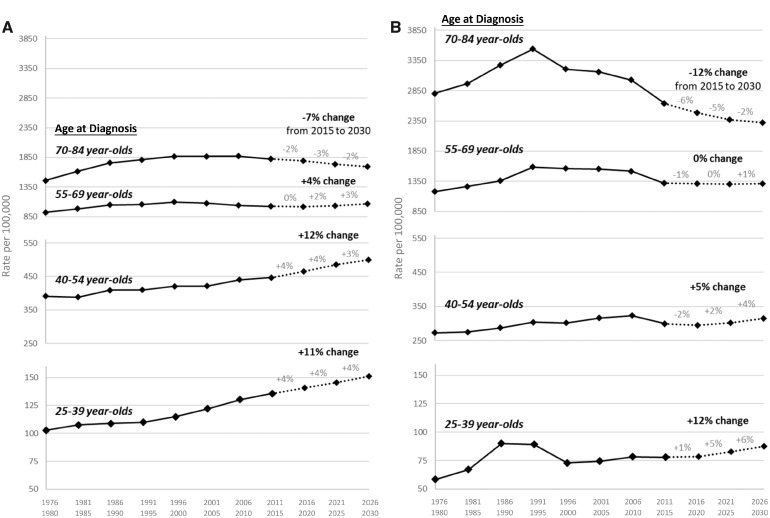
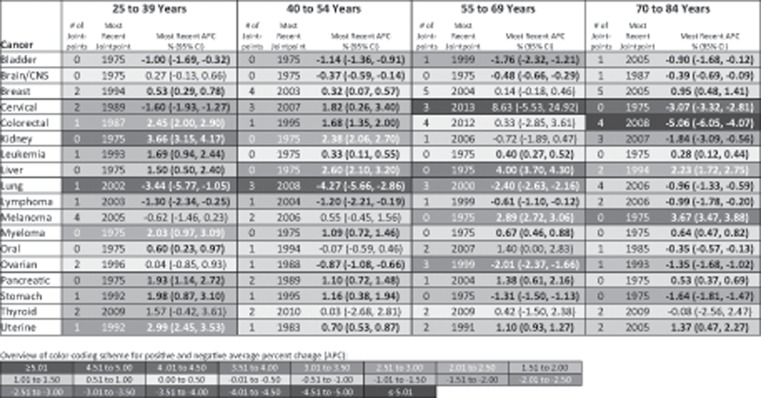
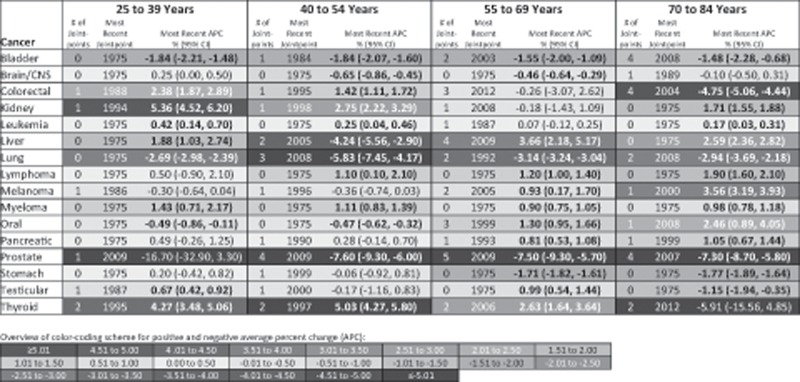
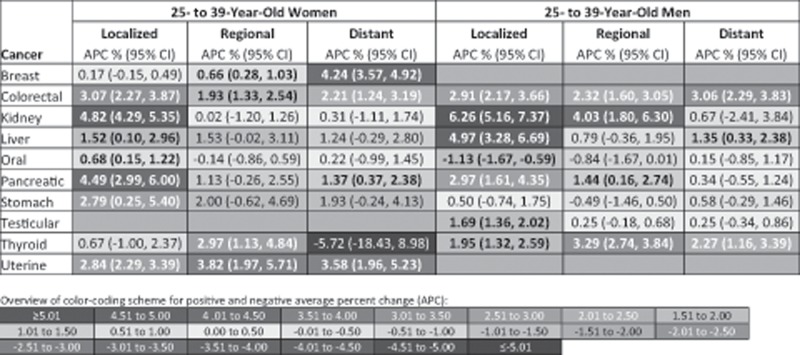
Results: Based on trends occurring after the most recent joinpoint inflection point, overall cancer incidence increased by 1.15% (95% CI = 1.01% to 1.28%) per year in 25- to 39-year-old women and by 0.46% (95% CI = 0.17% to 0.75%) per year in 25- to 39-year-old men; APCs were of much lower magnitude in the older age groups (eg, 70- to 84-year-old women APC = -0.31%, 95% CI = -0.42% to -0.20%). We forecasted that overall cancer incidence will increase by an additional 11% by 2030 in 25- to 39-year-old women, and by an additional 12% in 25- to 39-year-old men. Ten of the 18 cancers assessed in 25- to 39-year-old women and 7 of the 16 cancers in 25- to 39-year-old men have been statistically significantly increasing over time. We found that the increase in incidence for young adults is stage specific for some cancers (eg, only nonlocalized breast cancer has increased in 25- to 39-year-old women).
Conclusion: Cancer incidence is increasing in young adults, particularly in young women.
Figures
References
-
- Johnson RH, Chien FL, Bleyer A.. Incidence of breast cancer with distant involvement among women in the United States, 1976 to 2009. JAMA. 2013;309(8):800–805. - PubMed
-
- Sung H, Siegel RL, Rosenberg PS, Jemal A.. Emerging cancer trends among young adults in the USA: analysis of a population-based cancer registry. Lancet Public Health. 2019;4(3):e136–e147. - PubMed
-
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence—SEER 9 Regs Research Data, Nov 2017 Sub (1973-2015) <Katrina/Rita Population Adjustment>—Linked To County Attributes - Total U.S., 1969-2016 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2018. www.seer.cancer.gov. Based on November 2017 submission.
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous