

Diagnosis: gastric intestinal metaplasia - what to do next?
- PMID: 31415250
- PMCID: PMC6900998
- DOI: 10.1097/MOG.0000000000000576
Diagnosis: gastric intestinal metaplasia - what to do next?
Abstract
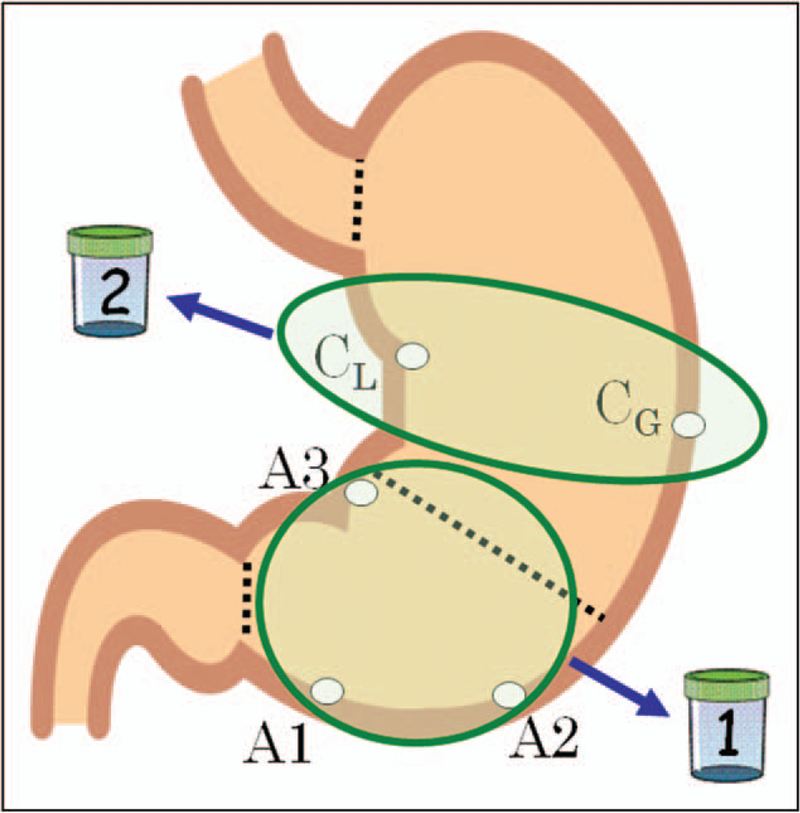
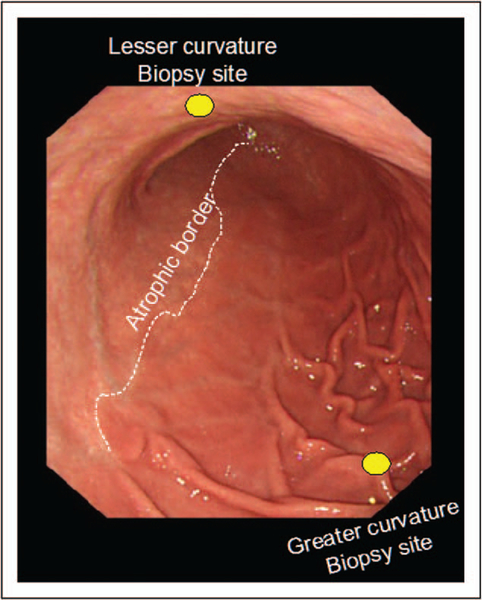
Purpose of review: One of the most vexing problems for gastroenterologists is what actions to take after receiving a histological diagnosis of gastric intestinal metaplasia. We approach the problem by starting with suggesting a biopsy protocol that ensures obtaining the biopsies required for diagnosis, assessing the status of the gastric mucosa, and effective communication with the pathologist and patient.
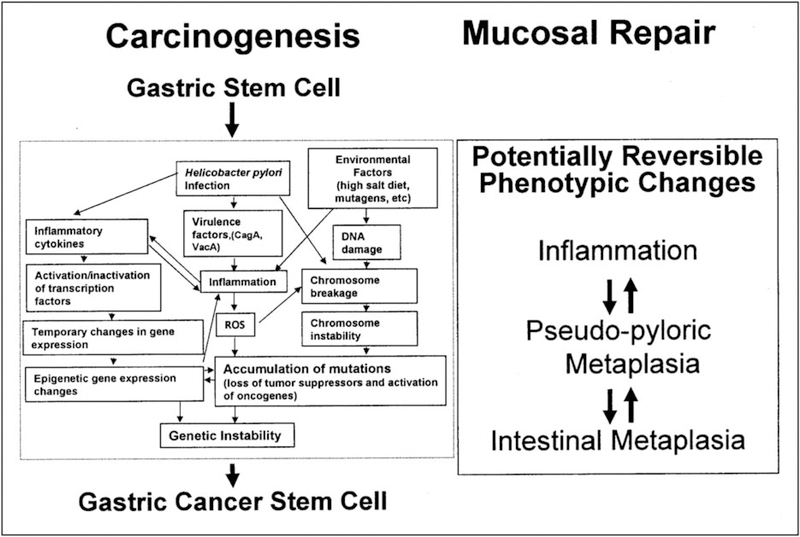
Recent findings: The rediscovery and integration of the long history of gastric damage and repair resulting in pseudopyloric metaplasia (called SPEM) into the thinking of investigators working with animal models of gastric cancer has resulted in improved ability to separate changes associated with benign repair from those associated with inflammation-associated gastric carcinogenesis.
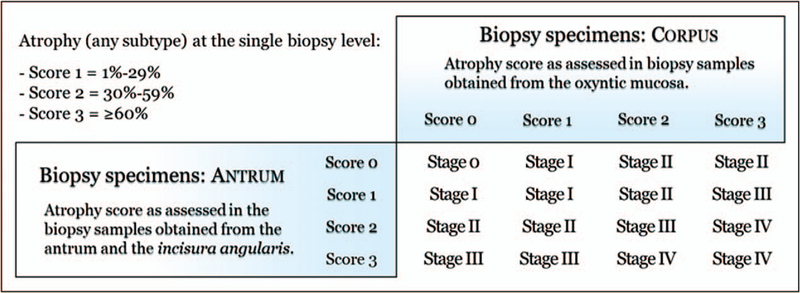
Summary: Gastric intestinal metaplasia is a potential reversible product of injury and repair and not directly connected with carcinogenesis. Intestinal metaplasia is a biomarker for prior gastric injury and repair. The risk of gastric cancer is best assessed in relation to the severity, extent, and, most importantly, the cause of the atrophic changes.
Conflict of interest statement
Conflicts of interest
M.R. has no conflicts to declare.
Figures
Similar articles
-
Guilt by association: intestinal metaplasia does not progress to gastric cancer.Curr Opin Gastroenterol. 2018 Nov;34(6):458-464. doi: 10.1097/MOG.0000000000000472. Curr Opin Gastroenterol. 2018. PMID: 30138135 Free PMC article. Review.
-
Pathological disorders of the gastric mucosa surrounding carcinomas and primary lymphomas.Am J Gastroenterol. 2001 Jun;96(6):1746-50. doi: 10.1111/j.1572-0241.2001.03868.x. Am J Gastroenterol. 2001. PMID: 11419824
-
Preinvasive neoplasia in the stomach: diagnosis and treatment.Clin Gastroenterol Hepatol. 2007 Sep;5(9):1018-23. doi: 10.1016/j.cgh.2007.07.004. Clin Gastroenterol Hepatol. 2007. PMID: 17825769
-
The gastric mucosa in gastric cancer patients in a low-incidence area.Eur J Gastroenterol Hepatol. 2006 Oct;18(10):1085-93. doi: 10.1097/01.meg.0000231753.58211.05. Eur J Gastroenterol Hepatol. 2006. PMID: 16957515
-
Helicobacter pylori associated gastric intestinal metaplasia: Treatment and surveillance.World J Gastroenterol. 2016 Jan 21;22(3):1311-20. doi: 10.3748/wjg.v22.i3.1311. World J Gastroenterol. 2016. PMID: 26811668 Free PMC article. Review.
Cited by
-
Metaplastic Paneth Cells in Extra-Intestinal Mucosal Niche Indicate a Link to Microbiome and Inflammation.Front Physiol. 2020 Mar 31;11:280. doi: 10.3389/fphys.2020.00280. eCollection 2020. Front Physiol. 2020. PMID: 32296343 Free PMC article. Review.
-
Investigating FGFR2 gene as a blood-based epigenetic biomarker in gastric cancer.Mol Biol Rep. 2024 Feb 1;51(1):253. doi: 10.1007/s11033-023-09082-0. Mol Biol Rep. 2024. PMID: 38302798
-
[Type A, Type B, and Non-atrophic Gastritis].Korean J Helicobacter Up Gastrointest Res. 2023 Jun;23(2):108-117. doi: 10.7704/kjhugr.2023.0015. Epub 2023 Jun 12. Korean J Helicobacter Up Gastrointest Res. 2023. PMID: 40502287 Free PMC article. Review. Korean.
-
Chronic Autoimmune Gastritis: Modern Diagnostic Principles.Diagnostics (Basel). 2021 Nov 15;11(11):2113. doi: 10.3390/diagnostics11112113. Diagnostics (Basel). 2021. PMID: 34829460 Free PMC article. Review.
-
Unveiling Cancer-Related Metaplastic Cells in Both Helicobacter pylori Infection and Autoimmune Gastritis.Gastroenterology. 2025 Jan;168(1):53-67. doi: 10.1053/j.gastro.2024.08.032. Epub 2024 Sep 3. Gastroenterology. 2025. PMID: 39236896
References
-
- Tan MC, Balakrishnan M, Graham DY. Gastric cancer worldwide except Japan In: Shiotani A, editor. Gastric cancer with special focus on studies from Japan. Singapore: Springer; 2018. pp. 17–28.
-
- Rugge M, Fassan M, Graham DY. Epidemiology of gastric cancer In: Strong VE, editor. Gastric cancer: principles and practice. Cham: Springer International Publishing; 2015. pp. 23–34.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
