

Mini-incisional entropion repair for correcting involutional entropion: Full description and surgical outcome
- PMID: 31415368
- PMCID: PMC6831266
- DOI: 10.1097/MD.0000000000016731
Mini-incisional entropion repair for correcting involutional entropion: Full description and surgical outcome
Abstract
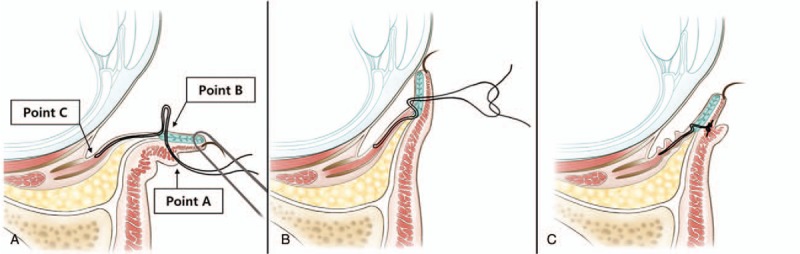
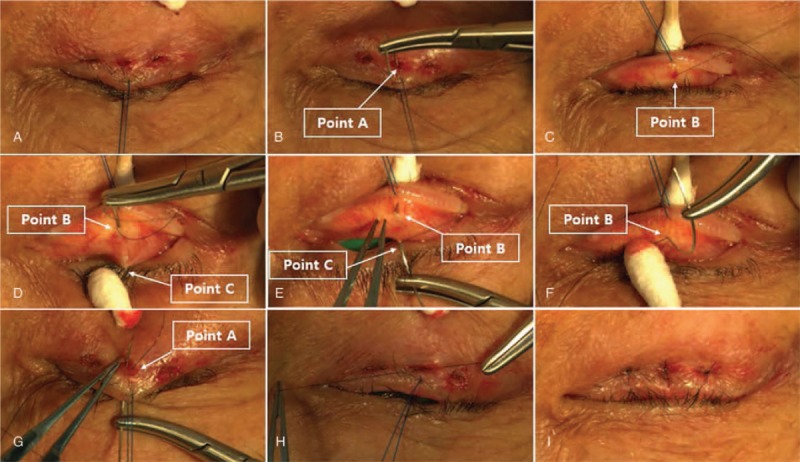
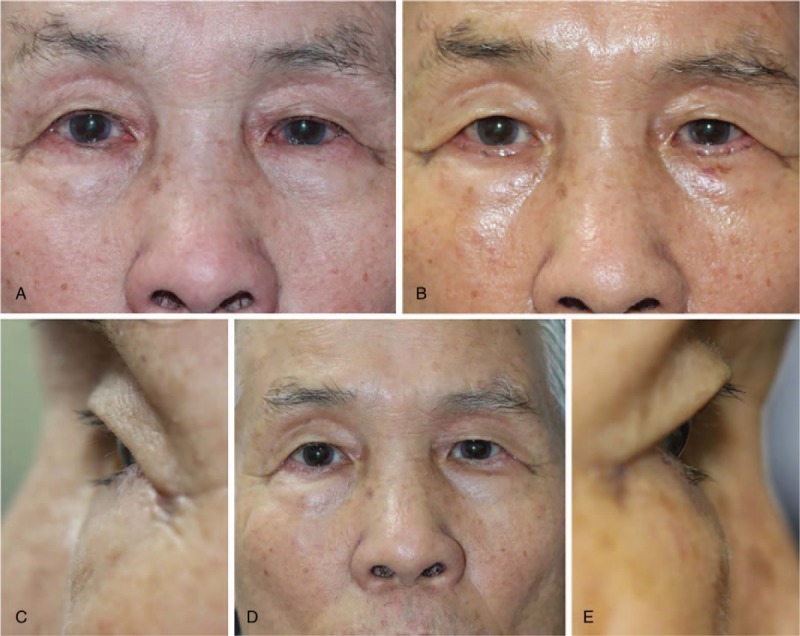
The aim of the study was to report the surgical outcome of mini-incisional correction method to treat involutional entropion.This is a retrospective interventional case series of 46 eyelids in 31 patients with involutional entropion and significant ocular irritation. In this technique, after turning the lower eyelid inside out, threads are introduced into it through the conjunctiva close to the inferior fornix. The lower lid retractor and tarsus are then connected using threads. These threads are applied at 3 locations of the lower eyelid and tightening them results in the eyelid being everted and the correction of entropion. Surgical success was defined as no contact between the eyelashes and the globe during forced closure of the eyelids. Surgical failure was defined as persistence of the eyelashes remaining in contact with the globe or cosmetic dissatisfaction.During the mean follow-up period of 22.1 months (range, 12-34 months), 43 of the eyelids (93.5%) were successfully corrected. Two patients (3 eyelids) experienced recurrence: 1 had involutional entropion combined with a cicatricial component, and the other had blepharospasm and apraxia of eyelid opening related to Parkinsonism. No postoperative complications such as overcorrection, suture-knot exposure, or ocular irritation were observed.Our mini-incisional entropion repair is based on reinforcement of the lower eyelid retractors using transconjunctival buried sutures. This technique is a quick, simple, and predictive for involutional entropion repair, and has a high success rate.
Figures
Similar articles
-
Involutional entropion repair with fornix sutures and lateral tarsal strip procedure.Ophthalmic Plast Reconstr Surg. 2001 Jul;17(4):281-7. doi: 10.1097/00002341-200107000-00008. Ophthalmic Plast Reconstr Surg. 2001. PMID: 11476179
-
Surgical correction of involutional lower lid entropion with lateral canthal eyelid block excision and imbrication of the capsulopalpebral ligament using non-buried non-resorbable imbricating sutures versus buried resorbable imbricating sutures.Orbit. 2019 Feb;38(1):7-12. doi: 10.1080/01676830.2018.1446538. Epub 2018 Mar 2. Orbit. 2019. PMID: 29498554
-
A small incision technique for repairing involutional lower eyelid entropion.Int Ophthalmol. 2020 Feb;40(2):281-285. doi: 10.1007/s10792-019-01172-y. Epub 2019 Oct 12. Int Ophthalmol. 2020. PMID: 31606822
-
Involutional lower eyelid entropion: causative factors and therapeutic management.Int Ophthalmol. 2019 Aug;39(8):1895-1907. doi: 10.1007/s10792-018-1004-1. Epub 2018 Oct 12. Int Ophthalmol. 2019. PMID: 30315389 Review.
-
Effective small-incision surgery for involutional lower eyelid entropion.Ophthalmology. 2000 Nov;107(11):1982-8. doi: 10.1016/s0161-6420(00)00358-4. Ophthalmology. 2000. PMID: 11054317 Review.
Cited by
-
Gender-Related Differences in Dry Eye Symptoms Following Involutional Ectropion and Entropion Surgery.Life (Basel). 2024 Jun 27;14(7):815. doi: 10.3390/life14070815. Life (Basel). 2024. PMID: 39063570 Free PMC article.
-
Changes in Lacrimal Punctum Position and Tear Meniscus Height after Correction of Horizontal Laxity in Involutional Lower Eyelid Entropion.J Ophthalmol. 2023 Jan 17;2023:4113151. doi: 10.1155/2023/4113151. eCollection 2023. J Ophthalmol. 2023. PMID: 36703702 Free PMC article.
-
Transcanthal Canthopexy for Involutional Lower Eyelid Entropion Corrects Horizontal Laxity.J Ophthalmol. 2024 Feb 13;2024:4694296. doi: 10.1155/2024/4694296. eCollection 2024. J Ophthalmol. 2024. PMID: 38379662 Free PMC article.
-
Outcomes of combined procedures compared to various single techniques for involutional entropion.Oman J Ophthalmol. 2023 Oct 18;16(3):439-445. doi: 10.4103/ojo.ojo_43_23. eCollection 2023 Sep-Dec. Oman J Ophthalmol. 2023. PMID: 38059104 Free PMC article.
-
Management of Eyelid Pathologies That Cause Corneal Lesions.Adv Exp Med Biol. 2025;1479:117-137. doi: 10.1007/5584_2024_837. Adv Exp Med Biol. 2025. PMID: 39656369 Review.
References
-
- Pereira MG, Rodrigues MA, Rodrigues SA. Eyelid entropion. Semin Ophthalmol 2010;25:52–8. - PubMed
-
- Marcet MM, Phelps PO, Lai JS. Involutional entropion: risk factors and surgical remedies. Curr Opin Ophthalmol 2015;26:416–21. - PubMed
-
- Damasceno RW, Osaki MH, Dantas PE, et al. Involutional entropion and ectropion of the lower eyelid: prevalence and associated risk factors in the elderly population. Ophthalmic Plast Reconstr Surg 2011;27:317–20. - PubMed
-
- Jones LT, Reeh MJ, Wobig JL. Senile entropion. A new concept for correction. Am J Ophthalmol 1972;74:327–9. - PubMed
-
- Benger RS, Musch DC. A comparative study of eyelid parameters in involutional entropion. Ophthalmic Plast Reconstr Surg 1989;5:281–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
