

An Educational Intervention for Acute Dizziness Care: A Randomized, Vignette-based Study
- PMID: 31415482
- PMCID: PMC6945771
- DOI: 10.1097/MAO.0000000000002338
An Educational Intervention for Acute Dizziness Care: A Randomized, Vignette-based Study
Abstract
Importance: Benign paroxysmal positional vertigo (BPPV) is a common cause of acute dizziness. Strong evidence exists for diagnosing BPPV using the Dix-Hallpike Test (DHT) and treating it with the canalith repositioning maneuver (CRM). Despite this, both are infrequently used in the emergency department (ED).
Objective: As an early method to evaluate a BPPV-focused educational intervention, we evaluated whether an educational intervention improved ED provider performance on hypothetical stroke and BPPV cases delivered by vignette.
Design: A randomized, controlled, educational intervention study in ED physicians. The intervention aimed to promote the appropriate use of the DHT and CRM. A BPPV vignette, a stroke-dizziness (safety) vignette, and vignette scoring schemes (higher scores indicating more optimal care) used previously established vignette methodology.
Setting: We recruited participants at the exhibitor hall of an emergency medicine annual meeting.
Participants: We recruited 48 emergency physicians. All were board certified or residency trained and board eligible. All were engaged in the active practice of emergency medicine. None were trainees.
Interventions: Intervention group: a narrated, educational presentation by computer followed by the clinical vignettes.
Control group: Received no educational intervention and completed the clinical vignettes-intended to mirror current clinician practice.
Main outcome measure: Primary endpoint: total score (out of 200 points) on a vignette-based scoring instrument assessing the performance of history, physical, and diagnostic testing on hypothetical stroke and BPPV cases.
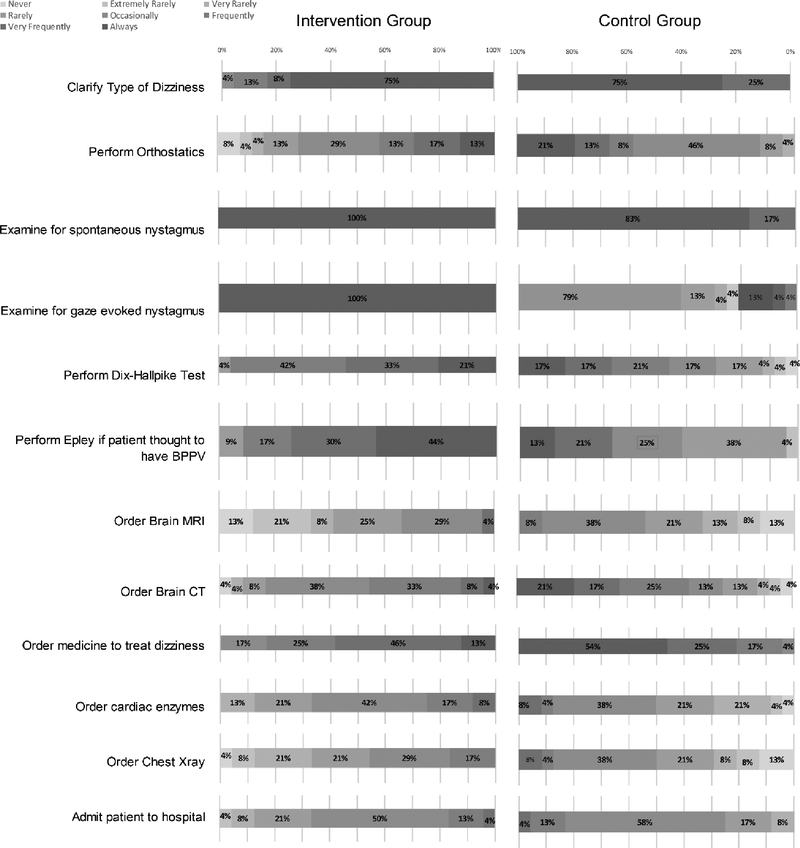
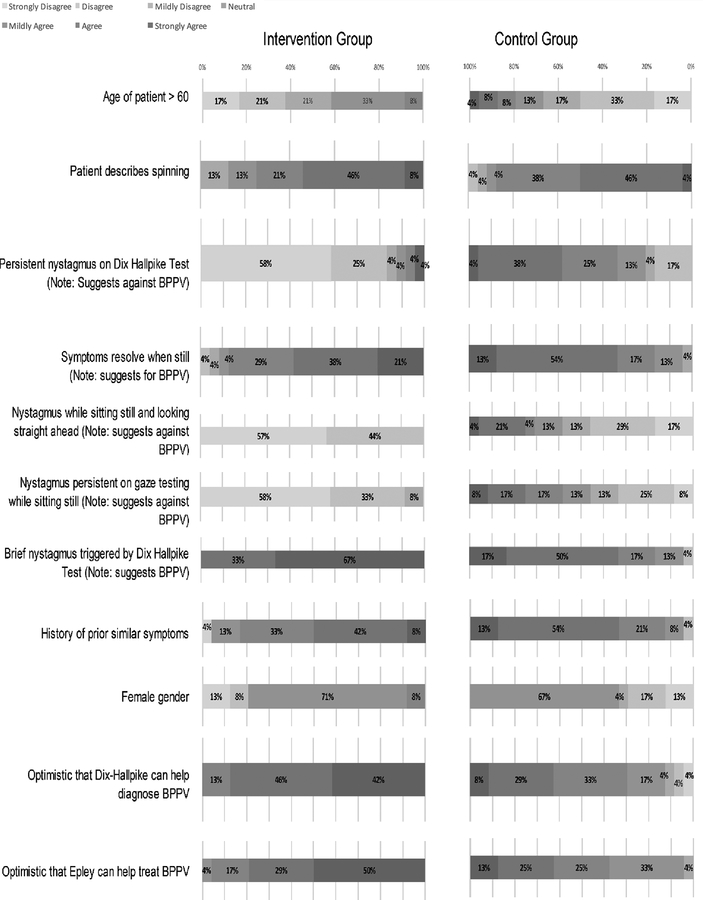
Results: The efficacy threshold was crossed at the interim analysis. The intervention group had higher performance scores compared with controls (113.2 versus 68.6, p < 0.00001). BPPV and safety subscores were both significantly higher in the intervention group. Sixty-two percent of the intervention group planned to use the DHT versus 29% of controls. After the vignette described characteristic BPPV nystagmus, 100% of the intervention group planned to use the CRM versus 17% of controls.
Conclusions and relevance: The educational intervention increased provider performance in dizziness vignettes, including more frequent appropriate use of the DHT/CRM. These findings indicate the intervention positively influenced planned behavior. Future work is needed to implement and evaluate this intervention in clinical practice.
Conflict of interest statement
Potential Conflicts of Interest
No authors have any conflicts of interest to report.
Figures
References
-
- Kerber KA, Meurer WJ, West BT and Mark Fendrick A, Dizziness presentations in US emergency departments, 1995–2004, Academic Emergency Medicine, 2008, 15(8):744–750. - PubMed
-
- Nedzelski J, Barber H and McIlmoyl L, Diagnoses in a dizziness unit, The Journal of otolaryngology, 1986, 15(2):101–104. - PubMed
-
- Kim J-S and Zee DS, Benign paroxysmal positional vertigo, New England Journal of Medicine, 2014, 370(12):1138–1147. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
