

Seasonality of antimicrobial resistance rates in respiratory bacteria: A systematic review and meta-analysis
- PMID: 31415656
- PMCID: PMC6695168
- DOI: 10.1371/journal.pone.0221133
Seasonality of antimicrobial resistance rates in respiratory bacteria: A systematic review and meta-analysis
Abstract
Background: Antimicrobial resistance (AMR) rates may display seasonal variation. However, it is not clear whether this seasonality is influenced by the seasonal variation of infectious diseases, geographical region or differences in antibiotic prescription patterns. Therefore, we assessed the seasonality of AMR rates in respiratory bacteria.
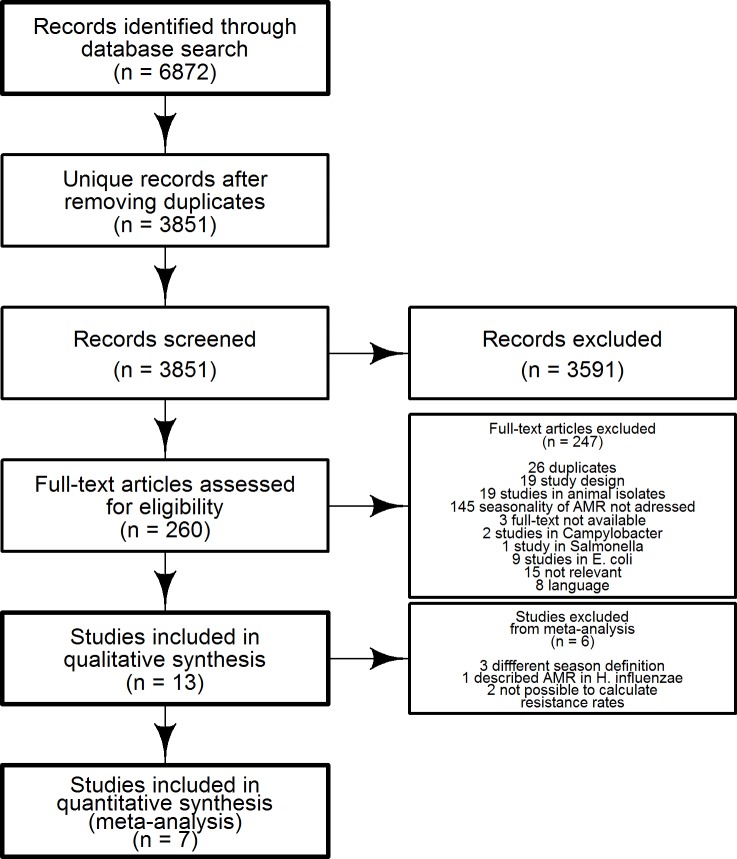
Methods: Seven electronic databases (Embase.com, Medline Ovid, Cochrane CENTRAL, Web of Science, Core Collection, Biosis Ovid, and Google Scholar), were searched for relevant studies from inception to Jun 25th, 2019. Studies describing resistance rates of Streptococcus pneumoniae and Haemophilus influenzae were included in this review. By using random-effects meta-analysis, pooled odd ratios of seasonal AMR rates were calculated using winter as the reference group. Pooled odd ratios were obtained by antibiotic class and geographical region.
Results: We included 13 studies, of which 7 were meta-analyzed. Few studies were done in H. influenzae, thus this was not quantitively analyzed. AMR rates of S. pneumoniae to penicillins were lower in other seasons than in winter with pooled OR = 0.71; 95% CI = 0.65-0.77; I2 = 0.0%, and to all antibiotics with pooled OR = 0.68; 95% CI = 0.60-0.76; I2 = 14.4%. Irrespective of geographical region, the seasonality of AMR rates in S. pneumoniae remained the same.
Conclusion: The seasonality of AMR rates could result from the seasonality of infectious diseases and its accompanied antibiotic use.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Similar articles
-
[Survey of nasopharyngeal carriage of Haemophilus influenzae and Streptococcus pneumoniae in infants at day care centers].Nihon Jibiinkoka Gakkai Kaiho. 2006 Dec;109(12):821-9. doi: 10.3950/jibiinkoka.109.821. Nihon Jibiinkoka Gakkai Kaiho. 2006. PMID: 17233437 Japanese.
-
Nasopharyngeal swabs of school children, useful in rapid assessment of community antimicrobial resistance patterns in Streptococcus pneumoniae and Haemophilus influenzae.J Clin Epidemiol. 2013 Jan;66(1):44-51. doi: 10.1016/j.jclinepi.2012.01.011. Epub 2012 Apr 26. J Clin Epidemiol. 2013. PMID: 22542022
-
[In vitro resistance rates of Streptococcus pneumoniae and Haemophilus influenzae clinical isolates to the antibiotics used in therapy].Mikrobiyol Bul. 2007 Jul;41(3):441-6. Mikrobiyol Bul. 2007. PMID: 17933256 Turkish.
-
[New spectra of resistance of the main bacteria of the respiratory tract].Arch Pediatr. 1998;5 Suppl 1:14s-17s. doi: 10.1016/s0929-693x(97)83482-3. Arch Pediatr. 1998. PMID: 10223155 Review. French.
-
[Macrolide antibiotics: Streptococcus pneumoniae and Haemophilus influenzae].Enferm Infecc Microbiol Clin. 1996 Oct;14(8):503-4. Enferm Infecc Microbiol Clin. 1996. PMID: 9011211 Review. Spanish. No abstract available.
Cited by
-
Physicochemical and microbiological characteristics of urban aerosols in Krakow (Poland) and their potential health impact.Environ Geochem Health. 2021 Nov;43(11):4601-4626. doi: 10.1007/s10653-021-00950-x. Epub 2021 Apr 29. Environ Geochem Health. 2021. PMID: 33913083 Free PMC article.
-
Vancomycin-resistant enterococci and coagulase-negative staphylococci prevalence among patients attending at Felege Hiwot Comprehensive Specialized Hospital, Bahir Dar, Ethiopia.PLoS One. 2021 Apr 8;16(4):e0249823. doi: 10.1371/journal.pone.0249823. eCollection 2021. PLoS One. 2021. PMID: 33831089 Free PMC article.
-
Improved penicillin susceptibility of Streptococcus pneumoniae and increased penicillin consumption in Japan, 2013-18.PLoS One. 2020 Oct 22;15(10):e0240655. doi: 10.1371/journal.pone.0240655. eCollection 2020. PLoS One. 2020. PMID: 33091045 Free PMC article.
-
Insights into Molecular Profiles, Resistance Patterns, and Virulence Traits of Staphylococci from Companion Dogs in Angola.Animals (Basel). 2025 Apr 4;15(7):1043. doi: 10.3390/ani15071043. Animals (Basel). 2025. PMID: 40218436 Free PMC article.
-
Highly resistant Salmonella Heidelberg circulating in broiler farms in southern Brazil.Braz J Microbiol. 2025 Mar;56(1):723-729. doi: 10.1007/s42770-024-01555-z. Epub 2024 Nov 6. Braz J Microbiol. 2025. PMID: 39500827
References
-
- World Health Organization. Pneumonia: WHO; 2016 [updated September 2016; cited 2017 Jun 19]. Available from:: http://www.who.int/mediacentre/factsheets/fs331/en/.
-
- Marco F. BE, García de LJ., Aguilard L. and the Spanish Surveillance Group for Respiratory Pathogens. Streptococcus pneumoniae in community-acquired respiratory tract infections in Spain: the impact of serotype and geographical, seasonal and clinical factors on its susceptibility to the most commonly prescribed antibiotics. Journal of Antimicrobial Chemotherapy. 2000;46:557–64. 10.1093/jac/46.4.557 - DOI - PubMed
-
- Siripongpreeda N, Hattasingh W, Amornvipas P, Eampokalap B, Sakoolgnam S, Pancharoen C, et al. Frequency and clinical course of invasive pneumococcal disease caused by penicillin-resistant and penicillin-sensitive Streptococcus pneumoniae in Thai children. Journal of the Medical Association of Thailand. 2010;93 (5):S1–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
