

The role of postoperative radiotherapy for completely resected pIIIA-N2 non-small cell lung cancer patients with different clinicopathological features: a systemic review and meta-analysis
- PMID: 31417638
- PMCID: PMC6692616
- DOI: 10.7150/jca.28680
The role of postoperative radiotherapy for completely resected pIIIA-N2 non-small cell lung cancer patients with different clinicopathological features: a systemic review and meta-analysis
Abstract
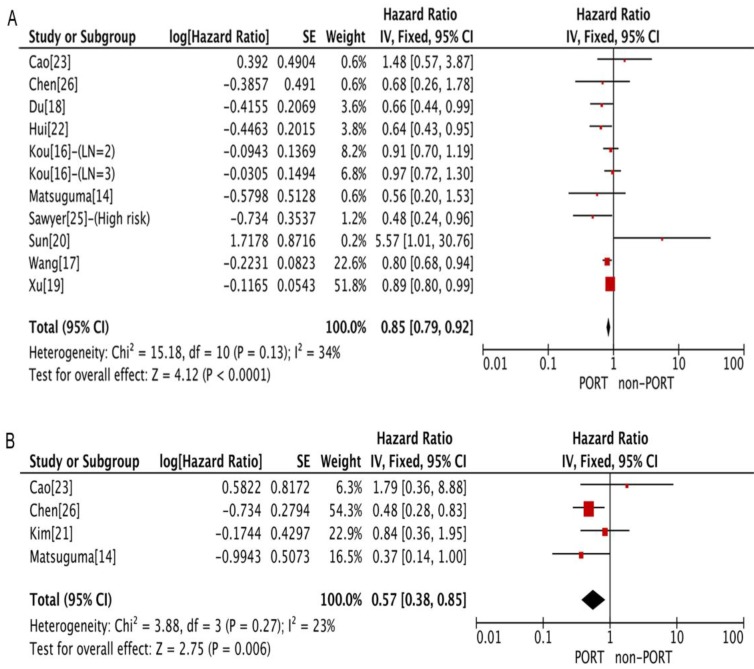
Background: The role of postoperative radiotherapy (PORT) in completely resected pathological stage IIIA-N2 (pIIIA-N2) non-small cell lung cancer (NSCLC) remains controversial. This meta-analysis aimed to assess the effect of PORT in patients with pIIIA-N2 NSCLC on the basis of clinicopathological features. Methods: The PubMed, PubMed Central (PMC), Embase, Web of Science, and Cochrane Library were searched for relevant studies. The main outcomes were overall survival (OS) and disease-free survival (DFS), which were compared using the hazard ratio (HR). Results: One randomized trial and 12 retrospective studies were eligible for the analysis. PORT significantly improved both OS [HR = 0.85; 95% confidence interval (CI): 0.79-0.92] and DFS (HR = 0.57; 95% CI: 0.38-0.85) compared with non-PORT treatment in patients with multiple N2 metastases or multiple N2 station involvement. No significant difference in either OS (HR = 1.03; 95% CI: 0.86-1.24) or DFS (HR = 1.08; 95% CI: 0.70-1.65) was found between PORT and non-PORT groups for patients with single N2 station involvement. No significant heterogeneity was observed. No significant differences in OS were observed between PORT and non-PORT groups for patients of different ages, sex, tumor sizes or pT stages, and histological types. Conclusions: The findings of this meta-analysis supported a role for PORT in patients with completely resected pIIIA-N2 NSCLC having multiple N2 metastases and favored withholding PORT to patients with single N2 station involvement. Further prospective randomized controlled trials are needed to confirm the findings.
Keywords: Clinicopathological features; Meta-analysis.; Non-small cell lung cancer; Postoperative radiotherapy; Stage IIIA-N2.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures





References
-
- Ettinger DS, Wood DE, Aisner DL. et al. Non-Small Cell Lung Cancer, Version 5.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017;15:504–35. - PubMed
-
- De Marinis F, Ciardiello F, Baas P. et al. 30 Immunotherapy in advanced NSCLC-from the 'tsunami' of therapeutic knowledge to a clinical practice algorithm: results from an international expert panel meeting of the Italian Association of Thoracic Oncology (AIOT) ESMO Open. 2018;3:e000298. - PMC - PubMed
-
- Goeckenjan G, Sitter H, Thomas M. et al. Prevention, diagnosis, therapy, and follow-up of lung cancer: Interdisciplinary guideline of the German Respiratory Society and the German Cancer Society. Pneumologie. 2011;65:e51–75. - PubMed
-
- Arriagada R, Bergman B, Dunant A. et al. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N Engl J Med. 2004;350:351–60. - PubMed
-
- Winton T, Livingston R, Johnson D. et al. Vinorelbine plus cisplatin vs. observation in resected non-small-cell lung cancer. N Engl J Med. 2005;352:2589–97. - PubMed
LinkOut - more resources
Full Text Sources
