

Biomarkers in Post-kala-azar Dermal Leishmaniasis
- PMID: 31417876
- PMCID: PMC6685405
- DOI: 10.3389/fcimb.2019.00228
Biomarkers in Post-kala-azar Dermal Leishmaniasis
Abstract
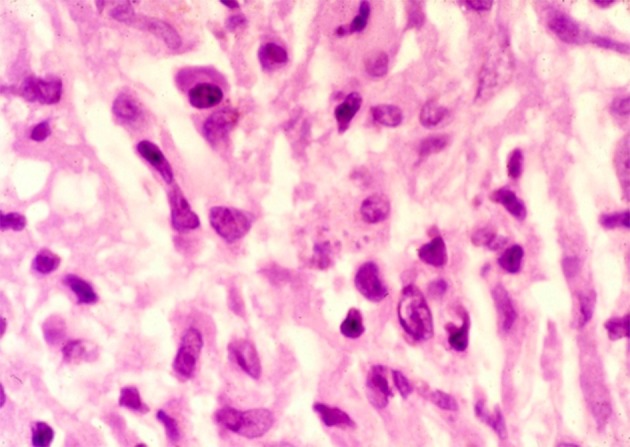
Post-kala-azar dermal leishmaniasis (PKDL) follows visceral leishmaniasis (VL, kala-azar) in 10-60% of cases. It is characterized by an asymptomatic skin rash, usually starting in the face and consisting of macules, papules, or nodules. Diagnosis is difficult in the field and is often made clinically. There is an extensive differential diagnosis, and parasitological confirmation is preferred particularly when drug treatment is considered. The response to treatment is difficult to assess as this may be slow and lesions take long to heal, thus possibly exposing patients unnecessarily to prolonged drug treatment. Biomarkers are needed; these may be parasitological (from microscopy, PCR), serological (from blood, or from the lesion), immunological (from blood, tissue), pathological (from cytology in a smear, histology in a biopsy), repeated clinical assessment (grading, photography), or combinations. In this paper, we will review evidence for currently used biomarkers and discuss promising developments.
Keywords: biochemical; biomarkers; clinical; immunological; parasitological; post-kala-azar dermal leishmaniasis.
Figures


References
-
- Abongomera C., Gatluak F., Buyze J., Ritmeijer K. (2016). A comparison of the effectiveness of sodium stibogluconate monotherapy to sodium stibogluconate and paromomycin combination for the treatment of severe post kala azar dermal leishmaniasis in south sudan—a retrospective cohort study. PLoS ONE. 11:e0163047 10.1371/journal.pone.0163047 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources