

Acute declines in estimated glomerular filtration rate on enalapril and mortality and cardiovascular outcomes in patients with heart failure with reduced ejection fraction
- PMID: 31420191
- PMCID: PMC7392085
- DOI: 10.1016/j.kint.2019.05.019
Acute declines in estimated glomerular filtration rate on enalapril and mortality and cardiovascular outcomes in patients with heart failure with reduced ejection fraction
Abstract
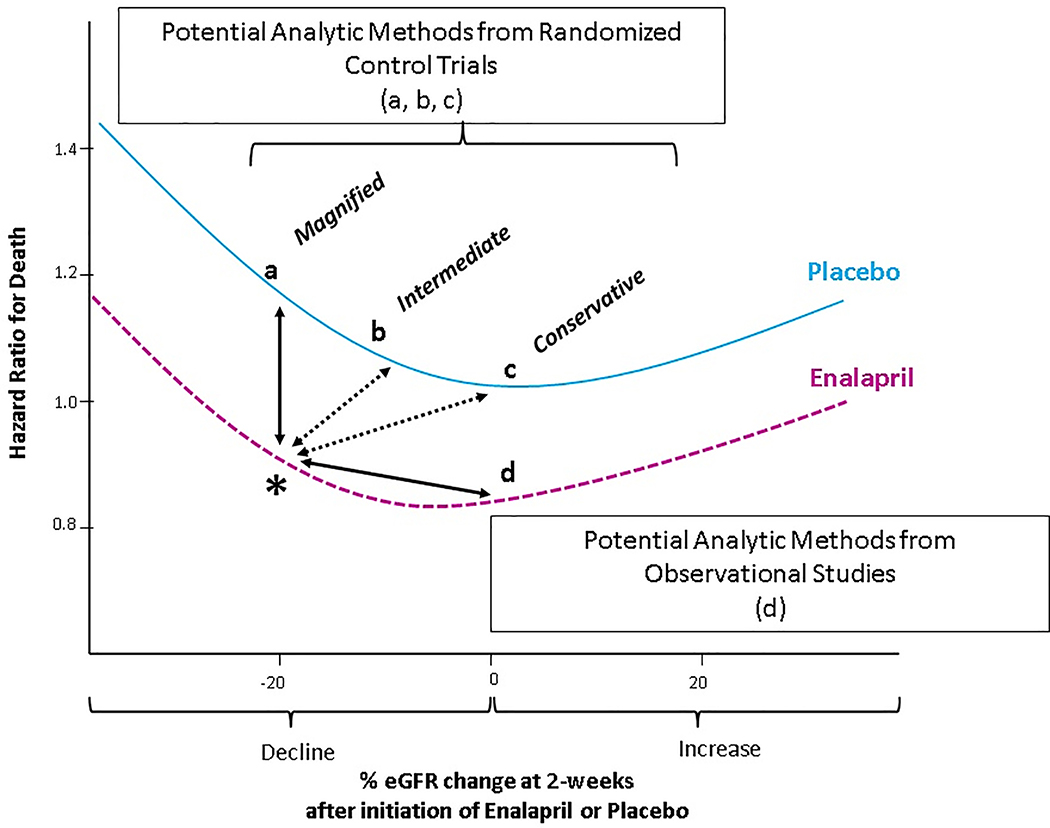
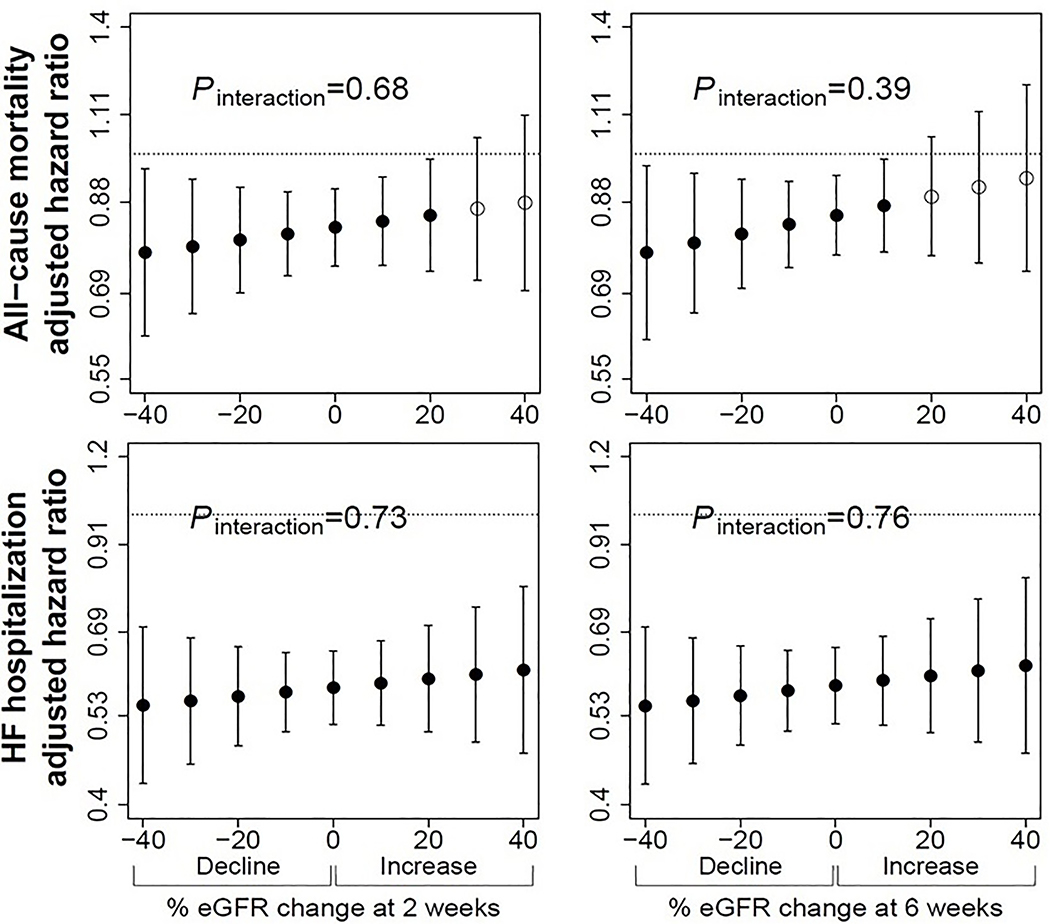
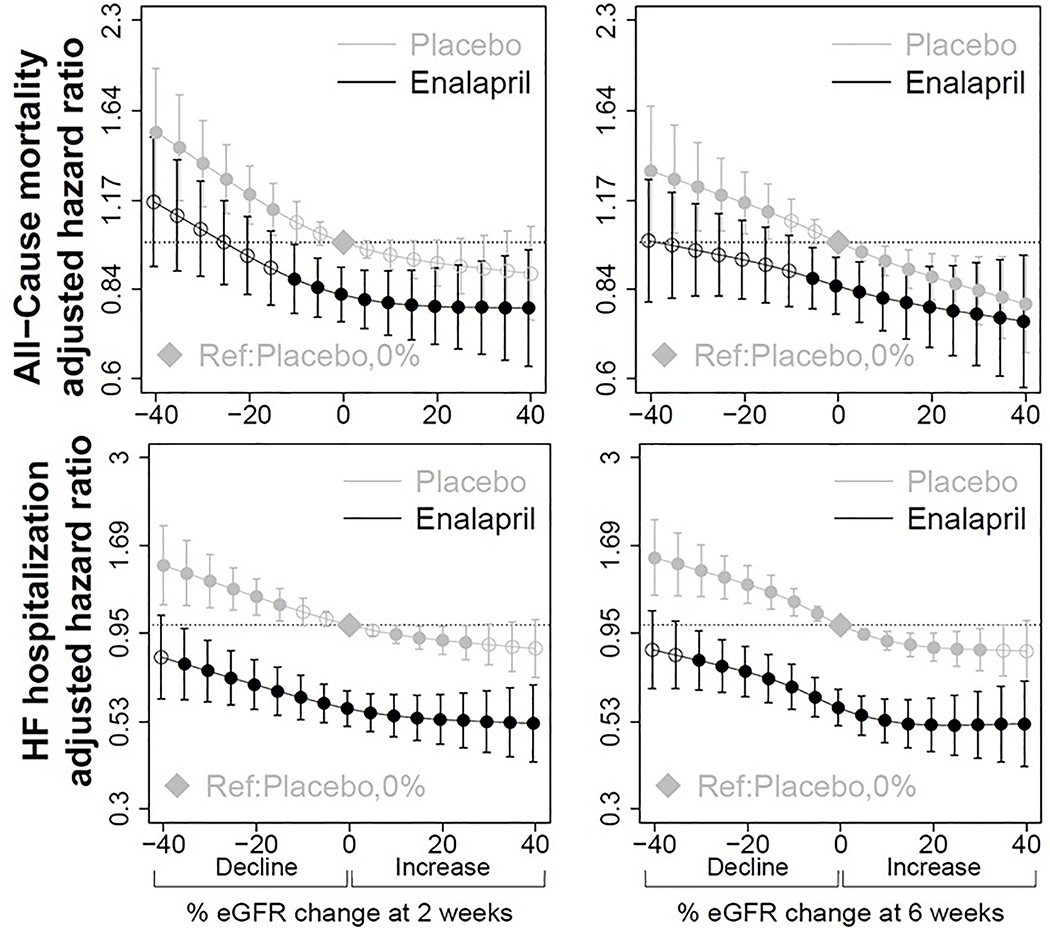
Angiotensin-converting enzyme inhibitors are beneficial in heart failure with reduced ejection fraction but are associated with acute declines in estimated glomerular filtration rate (eGFR). Prior studies evaluating thresholds of eGFR decline while using angiotensin-converting enzyme inhibitors in heart failure with reduced ejection have not taken into account this medication-driven decline. Here we used data from the Studies of Left Ventricular Dysfunction (SOLVD) trial of 6245 patients and performed Cox proportional hazards regression models to calculate hazard ratios of all-cause mortality and heart failure hospitalization-associated with percent eGFR decline at two- and six-weeks after randomization to enalapril versus placebo. In reference to placebo with equal degree of percent eGFR decline, any eGFR decline in the enalapril arm was associated with lower hazard of both outcomes. Under a conservative estimate using zero percent eGFR decline in the placebo arm as the reference, up to a 10% decline with enalapril was associated with mortality benefit (hazard ratio 0.87 [95% confidence interval 0.77, 0.99]) while up to a 35% decline was associated with decreased risk of heart failure hospitalization (0.78 [0.61, 0.98]). Under an intermediate estimate, up to a 15% decline with enalapril was associated with a mortality benefit (0.86 [0.77, 0.97]) and all levels of eGFR decline were associated with decreased risk of heart failure hospitalization. There was no percent eGFR decline, including up to 40%, in any models at either two- or six-weeks where enalapril was associated with higher mortality risk. Thus, in patients with reduced ejection fraction heart failure, enalapril is associated with decreased risk of mortality and heart failure hospitalizations. Hence, compelling reasons beyond moderate eGFR decline ought to be considered before its use is withdrawn.
Keywords: ACE inhibitor; SOLVD; cardiorenal syndrome; heart failure; kidney function decline.
Copyright © 2019 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
"Permissive AKI" with treatment of heart failure.Kidney Int. 2019 Nov;96(5):1066-1068. doi: 10.1016/j.kint.2019.07.003. Kidney Int. 2019. PMID: 31648696
References
-
- Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). The New England journal of medicine. 1987;316(23):1429–1435. - PubMed
-
- Carson P, Tognoni G, Cohn JN. Effect of Valsartan on hospitalization: results from Val-HeFT. Journal of cardiac failure. 2003;9(3):164–171. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128(16):e240–327. - PubMed
-
- Konstam MA, Rousseau MF, Kronenberg MW, et al. Effects of the angiotensin converting enzyme inhibitor enalapril on the long-term progression of left ventricular dysfunction in patients with heart failure. SOLVD Investigators. Circulation. 1992;86(2):431–438. - PubMed
-
- Konstam MA, Kronenberg MW, Rousseau MF, et al. Effects of the angiotensin converting enzyme inhibitor enalapril on the long-term progression of left ventricular dilatation in patients with asymptomatic systolic dysfunction. SOLVD (Studies of Left Ventricular Dysfunction) Investigators. Circulation. 1993;88(5 Pt 1):2277–2283. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
