

Comment
doi: 10.1681/ASN.2019050550.
Epub 2019 Aug 16.
Authors' Reply
Affiliations
- PMID: 31420405
- PMCID: PMC6727257
- DOI: 10.1681/ASN.2019050550
Item in Clipboard
Comment
Authors' Reply
J Am Soc Nephrol.
2019 Sep.
No abstract available
Figures
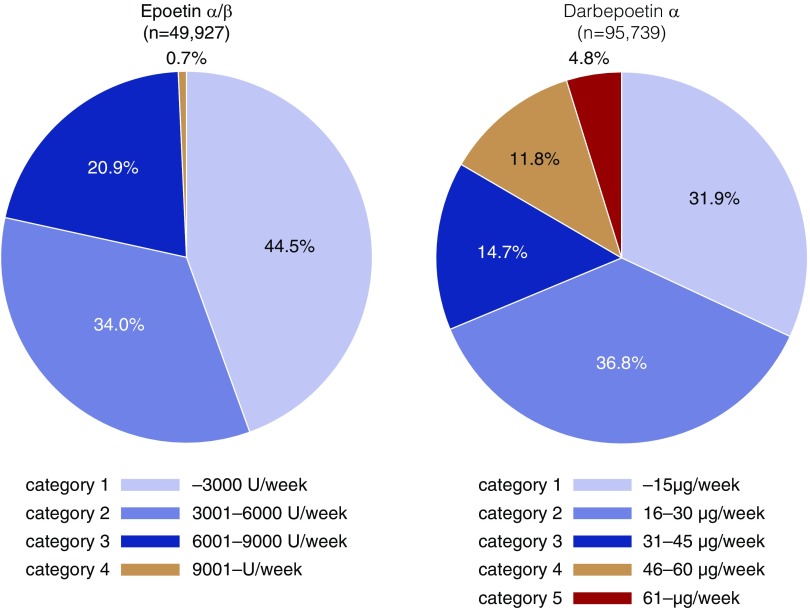
Higher doses of ESA are prescribed for patients taking DPO-α (i.e., category 4 and 5) compared with those taking EPO-α/β. The range of ESA doses in each category is based on the dose conversion ratio (EPO/DPO=200).
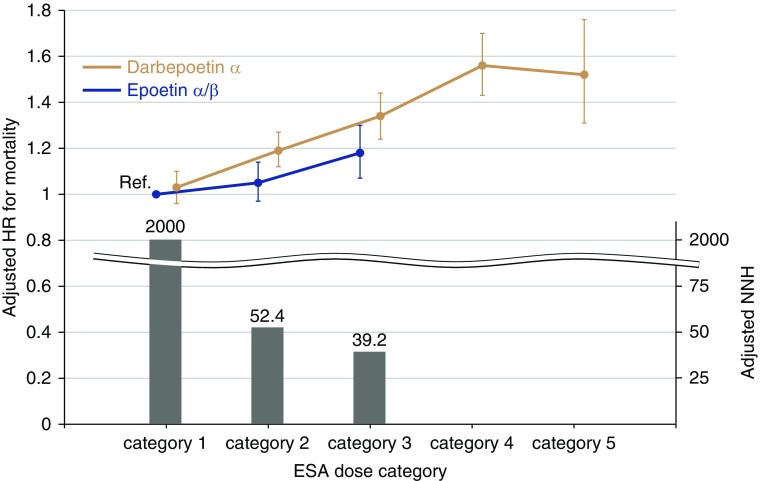
Mortality rates are elevated in patients treated with DPO-α except for those in ESA dose category 1. The Cox proportional hazards model was adjusted for age, sex, body mass index, predialysis systolic BP, dialysis duration, dialysis vintage, single-pool Kt/V, diabetes mellitus, a history of cardiovascular diseases, laboratory data (albumin, urea nitrogen, C-reactive protein, hemoglobin, ferritin, albumin-adjusted calcium, phosphate, and parathyroid hormone), standardized erythropoietin resistance index, and facility indicators. The patients taking EPO-α/β in category 1 were treated as a reference group. The bar graph denotes the adjusted 2-year numbers needed to harm for all-cause death, which was calculated from the reciprocal of the adjusted absolute risk difference between patients taking EPO-α/β and those taking DPO-α in each ESA dose category. HR, hazard ratio; NNH, number needed to harm; Ref., reference.
Comment on
-
Analysis of Other Confounding Factors Is Mandatory before Considering That Long-Acting Erythropoiesis Stimulating Agents Are Deleterious to Patients on Dialysis.J Am Soc Nephrol. 2019 Sep;30(9):1771. doi: 10.1681/ASN.2019050505. Epub 2019 Aug 16. J Am Soc Nephrol. 2019. PMID: 31420408 Free PMC article. No abstract available.
References
-
- Besarab A, Bolton WK, Browne JK, Egrie JC, Nissenson AR, Okamoto DM, et al. : The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med 339: 584–590, 1998 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
