

Integrated clinical, histopathological, and molecular data analysis of 190 central nervous system germ cell tumors from the iGCT Consortium
- PMID: 31420671
- PMCID: PMC6917411
- DOI: 10.1093/neuonc/noz139
Integrated clinical, histopathological, and molecular data analysis of 190 central nervous system germ cell tumors from the iGCT Consortium
Abstract
Background: We integrated clinical, histopathological, and molecular data of central nervous system germ cell tumors to provide insights into their management.
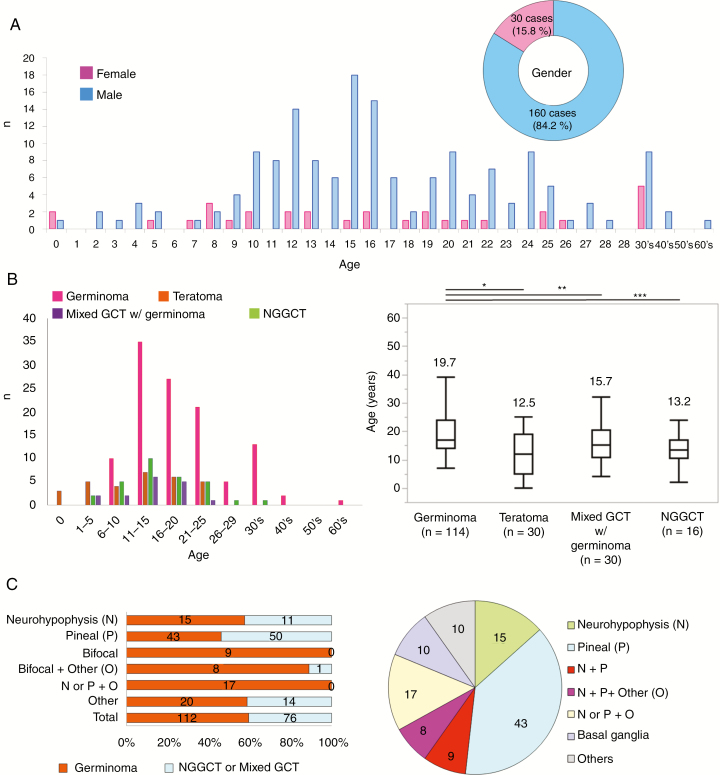
Methods: Data from the Intracranial Germ Cell Tumor Genome Analysis (iGCT) Consortium were reviewed. A total of 190 cases were classified as primary germ cell tumors (GCTs) based on central pathological reviews.
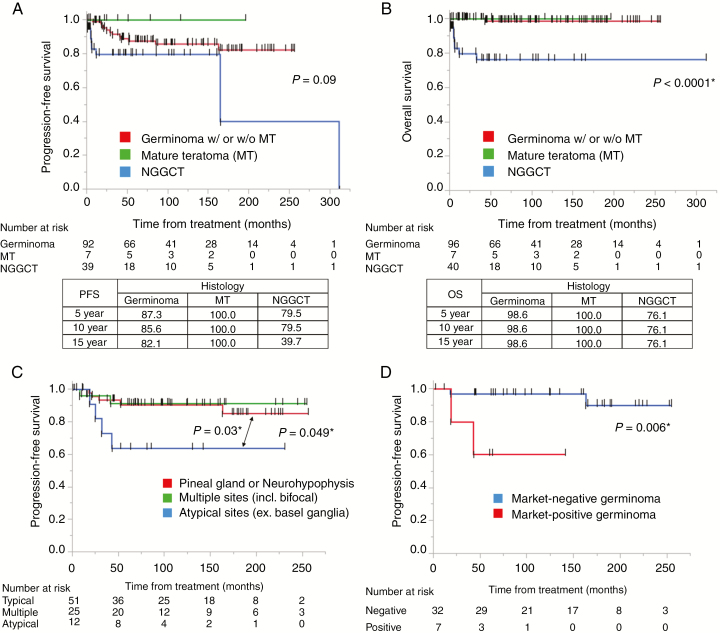
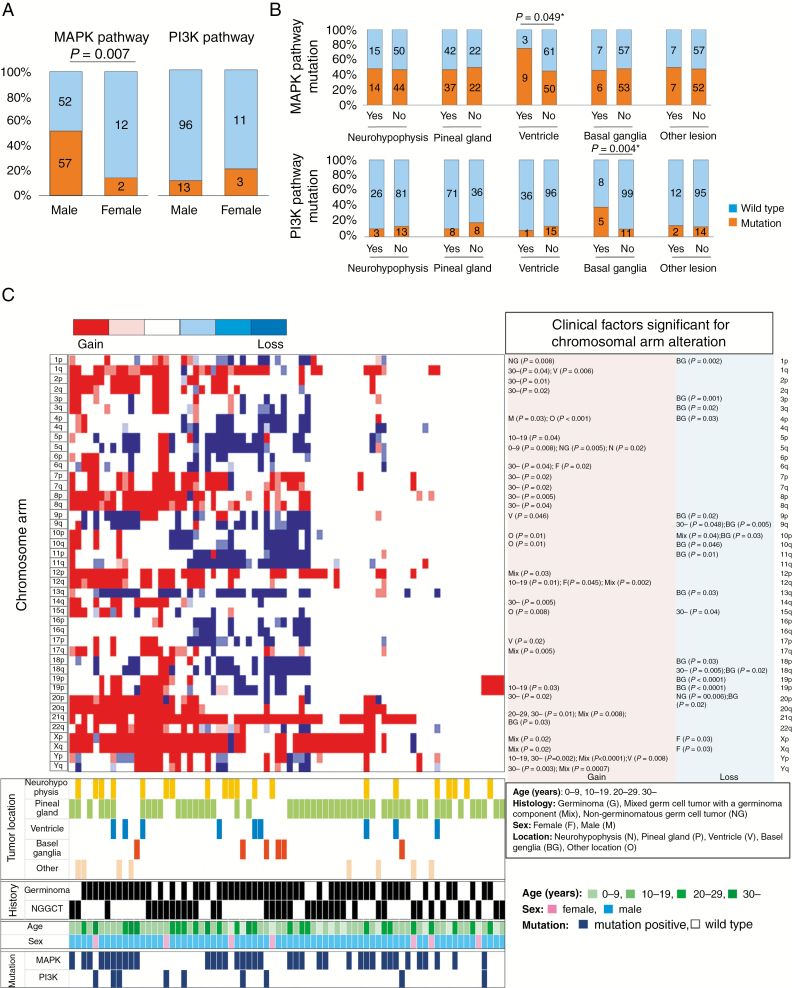
Results: All but one of the cases that were bifocal (neurohypophysis and pineal glands) and cases with multiple lesions including neurohypophysis or pineal gland were germinomas (34 of 35). Age was significantly higher in patients with germinoma than other histologies. Comparison between tumor marker and histopathological diagnoses showed that 18.2% of histopathologically diagnosed germinomas were marker positive and 6.1% of non-germinomatous GCTs were marker negative, suggesting a limitation in the utility of markers or histopathology alone using small specimens for diagnosis. Comparison between local and central histopathological diagnoses revealed a discordance of 12.7%. Discordance was significantly less frequent in biopsy cases, implying difficulty in detecting all histopathological components of heterogeneous GCTs. Germinomas at the typical sites (neurohypophysis or pineal gland) showed a better progression-free survival than those at atypical sites (P = 0.03). A molecular clinical association study revealed frequent mitogen-activated protein kinase (MAPK) pathway mutations in males (51.4% vs 14.3%, P = 0.007), and phosphatidylinositol-3 kinase/mammalian target of rapamycin (PI3K/mTOR) pathway mutations in basal ganglia cases (P = 0.004). Basal ganglia cases also had frequent chromosomal losses. Some chromosomal aberrations (2q, 8q gain, 5q, 9p/q, 13q, 15q loss) showed potential prognostic significance.
Conclusions: The in-depth findings of this study regarding clinical and molecular heterogeneity will increase our understanding of the pathogenesis of this enigmatic tumor.
Keywords: germ cell tumor; pathological diagnosis; prognosis, tumor marker; rare disease.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Shibui S. Report of brain tumor registry of Japan (2001–2004). Neurol Med Chir. 2014;54(suppl. 1) :1–102.
-
- Louis D, Ohgaki H, Wiestler O, Cavenee W.. WHO Classification of Tumours of the Central Nervous System. Revised 4th ed. Lyon, France: International Agency for Research on Cancer; 2016.
-
- Goldman S, Bouffet E, Fisher PG, et al. . Phase II trial assessing the ability of neoadjuvant chemotherapy with or without second-look surgery to eliminate measurable disease for nongerminomatous germ cell tumors: a Children’s Oncology Group Study. J Clin Oncol. 2015;33(22):2464–2471. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
