

Prescribing Associated with High-Risk Opioid Exposures Among Non-cancer Chronic Users of Opioid Analgesics: a Social Network Analysis
- PMID: 31420823
- PMCID: PMC6848735
- DOI: 10.1007/s11606-019-05114-3
Prescribing Associated with High-Risk Opioid Exposures Among Non-cancer Chronic Users of Opioid Analgesics: a Social Network Analysis
Abstract
Background: The continued rise in fatalities from opioid analgesics despite a steady decline in the number of individual prescriptions directing ≥ 90 morphine milligram equivalents (MME)/day may be explained by patient exposures to redundant prescriptions from multiple prescribers.
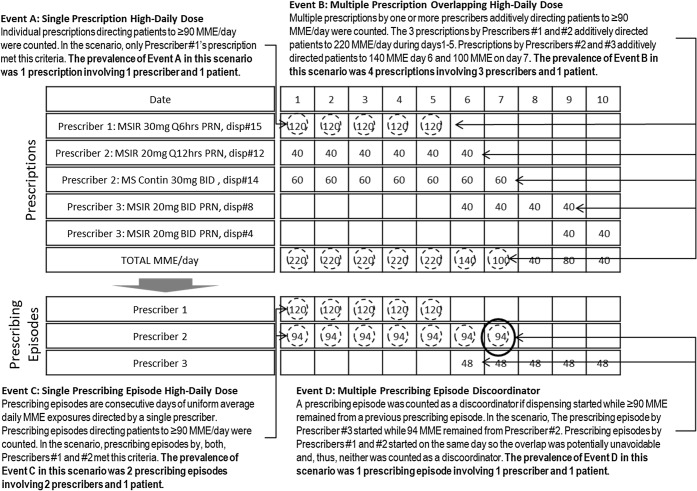
Objectives: We evaluated prescribers' specialty and social network characteristics associated with high-risk opioid exposures resulting from single-prescriber high-daily dose prescriptions or multi-prescriber discoordination.
Design: Retrospective cohort study.
Participants: A cohort of prescribers with opioid analgesic prescription claims for non-cancer chronic opioid users in an Illinois Medicaid managed care program in 2015-2016.
Main measures: Per prescriber rates of single-prescriber high-daily-dose prescriptions or multi-prescriber discoordination.
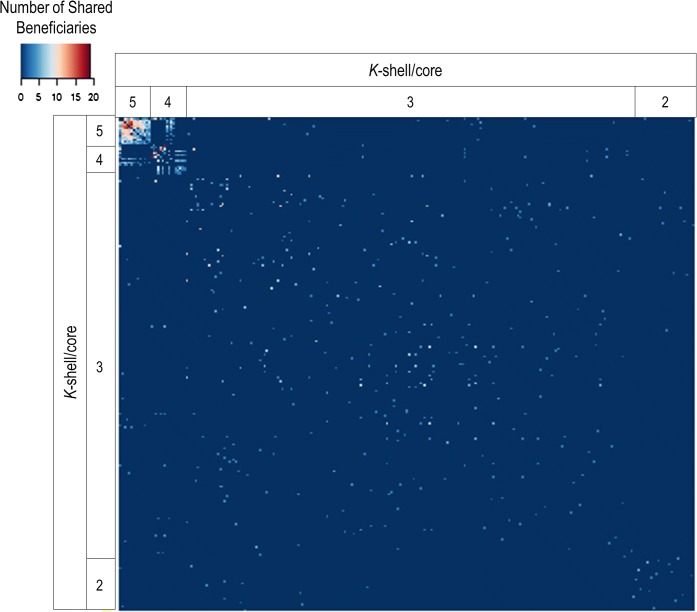
Key results: For 2280 beneficiaries, 36,798 opioid prescription claims were submitted by 3532 prescribers. Compared to 3% of prescriptions (involving 6% of prescribers and 7% of beneficiaries) that directed ≥ 90 MME/day, discoordination accounted for a greater share of high-risk exposures-13% of prescriptions (involving 23% of prescribers and 24% of beneficiaries). The following specialties were at highest risk of discoordinated prescribing compared to internal medicine: dental (incident rate ratio (95% confidence interval) 5.9 (4.6, 7.5)), emergency medicine (4.7 (3.8, 5.8)), and surgical subspecialties (4.2 (3.0, 5.8)). Social network analysis identified 2 small interconnected prescriber communities of high-volume pain management specialists, and 3 sparsely connected groups of predominantly low-volume primary care or emergency medicine clinicians. Using multivariate models, we found that the sparsely connected sociometric positions were a risk factor for high-risk exposures.
Conclusion: Low-volume prescribers in the social network's periphery were at greater risk of intended or discoordinated prescribing than interconnected high-volume prescribers. Interventions addressing discoordination among low-volume opioid prescribers in non-integrated practices should be a priority. Demands for enhanced functionality and integration of Prescription Drug Monitoring Programs or referrals to specialized multidisciplinary pain management centers are potential policy implications.
Keywords: Medicaid; care discoordination; epidemiology; harm reduction; opioid analgesic prescribing; social network analysis.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- 2018 Annual Surveillance Report of Drug-Related Risks and Outcomes -- United States. Centers for Disease Control and Prevention, US Department of Health and Human Services. Published August 31, 2018. https://www.cdc.gov/drugoverdose/pdf/pubs/2018-cdc-drug-surveillance-rep.... Accessed 1 May 2019
-
- Prescribing patterns of schedule II opioids in California Workers’ Compensation. 2011. http://www.cwci.org/document.php?file=1438.pdf. Accessed 1 May 2019
-
- Chang HY, Murimi IB, Jones CM, Alexander GC. Relationship between high-risk patients receiving prescription opioids and high-volume opioid prescribers. Addiction 2017. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
