

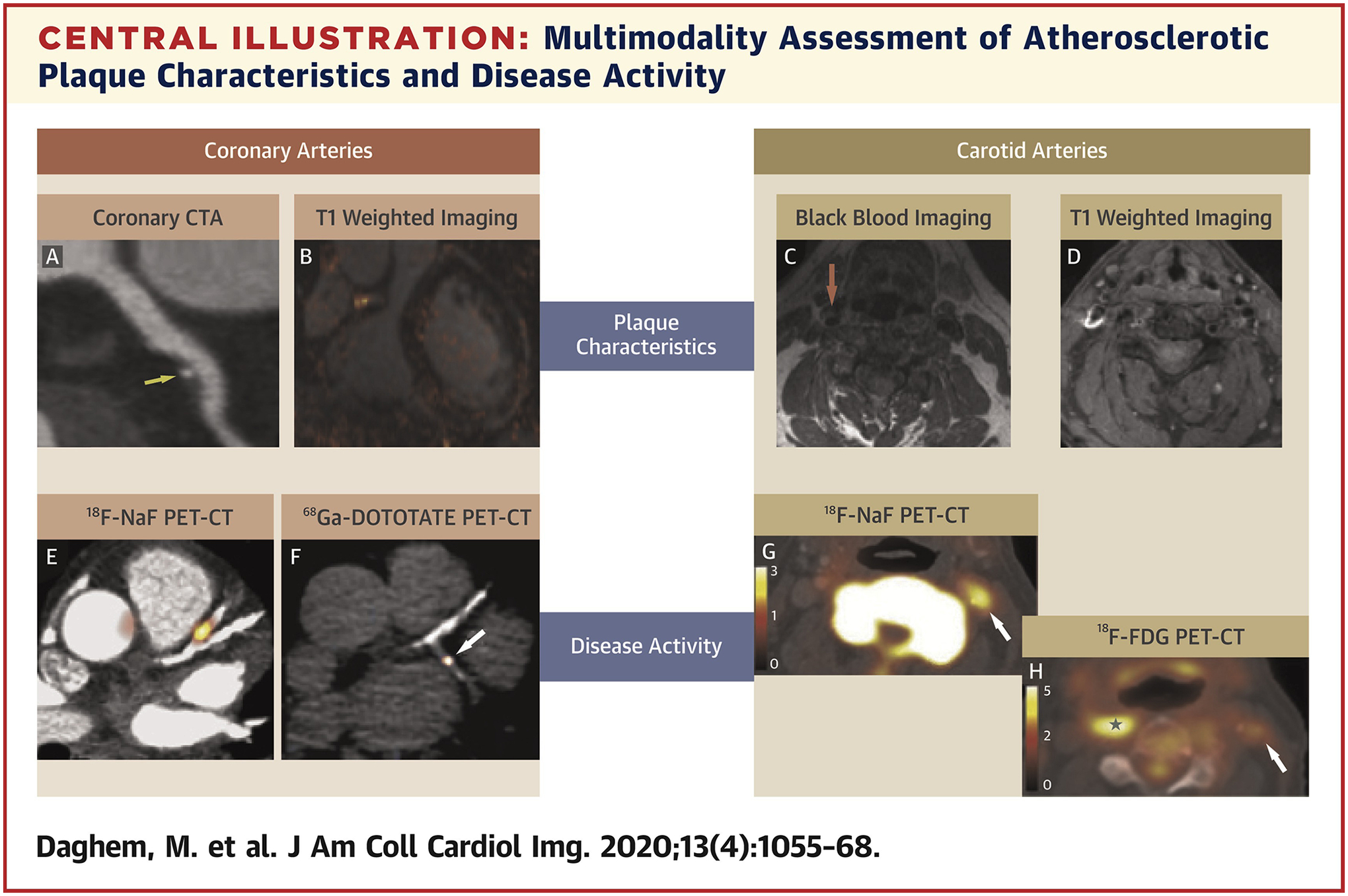
Noninvasive Imaging to Assess Atherosclerotic Plaque Composition and Disease Activity: Coronary and Carotid Applications
- PMID: 31422147
- PMCID: PMC10661368
- DOI: 10.1016/j.jcmg.2019.03.033
Noninvasive Imaging to Assess Atherosclerotic Plaque Composition and Disease Activity: Coronary and Carotid Applications
Abstract
Cardiovascular disease is one of the leading causes of mortality and morbidity worldwide. Atherosclerosis imaging has traditionally focused on detection of obstructive luminal stenoses or measurements of plaque burden. However, with advances in imaging technology it has now become possible to noninvasively interrogate plaque composition and disease activity, thereby differentiating stable from unstable patterns of disease and potentially improving risk stratification. This manuscript reviews multimodality imaging in this field, focusing on carotid and coronary atherosclerosis and how these novel techniques have the potential to complement current imaging assessments and improve clinical decision making.
Keywords: atherosclerosis; plaque burden; positron emission tomography; vulnerable plaque.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Relationship of atherosclerosis in young men to serum lipoprotein cholesterol concentrations and smoking. A preliminary report from the Patho-biological Determinants of Atherosclerosis in Youth (PDAY) Research Group. JAMA 1990;264: 3018–24. - PubMed
-
- Fihn SD, Blankenship JC, Alexander KP, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2014;64:1929–49. - PubMed
-
- Jonas DE, Feltner C, Amick HR, et al. Screening for asymptomatic carotid artery stenosis: a systematic review and meta-analysis for the U.S. Preventive Services Task Force. Ann Intern Med 2014;161:336–46. - PubMed
-
- Halliday A, Mansfield A, Marro J, et al. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet 2004;363:1491–502. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
