

Lisfranc fracture-dislocations: current management
- PMID: 31423327
- PMCID: PMC6667981
- DOI: 10.1302/2058-5241.4.180076
Lisfranc fracture-dislocations: current management
Abstract
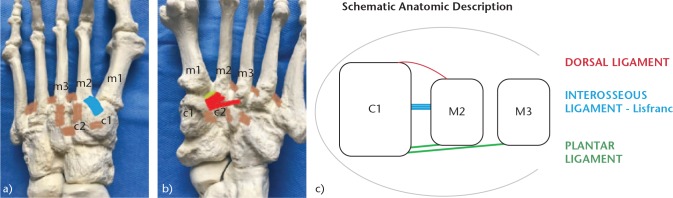
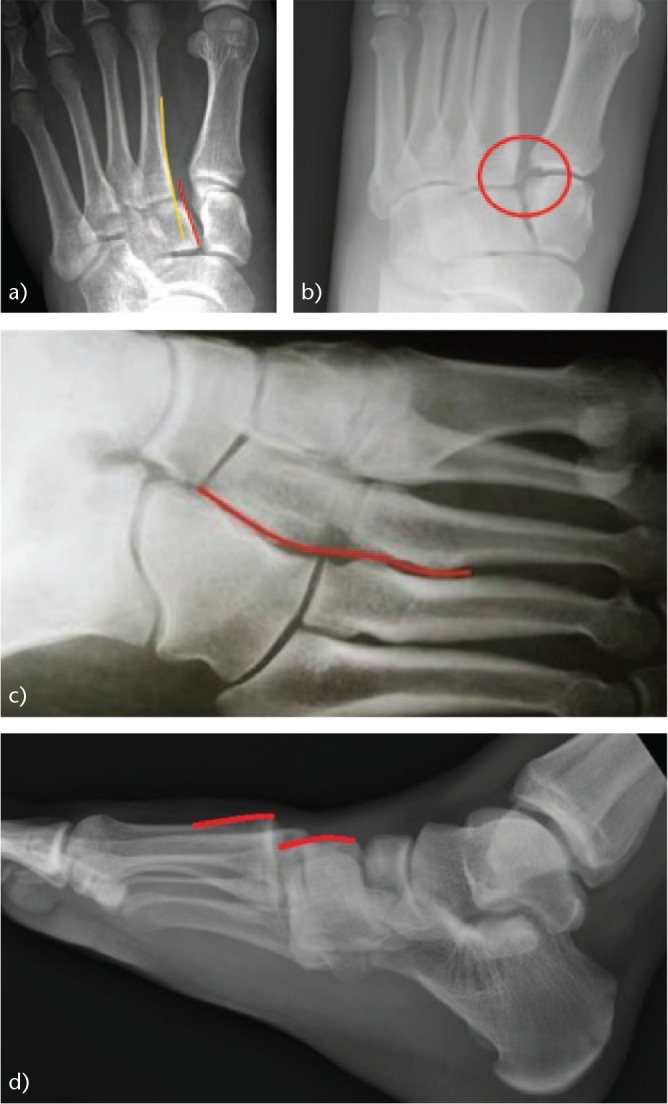
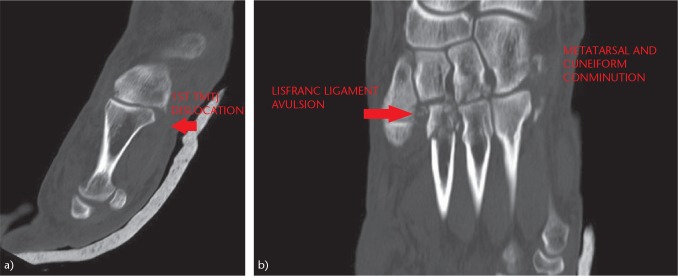
It is essential to know and understand the anatomy of the tarsometatarsal (TMT) joint (Lisfranc joint) to achieve a correct diagnosis and proper treatment of the injuries that occur at that level.Up to 20% of Lisfranc fracture-dislocations go unnoticed or are diagnosed late, especially low-energy injuries or purely ligamentous injuries. Severe sequelae such as post-traumatic osteoarthritis and foot deformities can create serious disability.We must be attentive to the clinical and radiological signs of an injury to the Lisfranc joint and expand the study with weight-bearing radiographs or computed tomography (CT) scans.Only in stable lesions and in those without displacement is conservative treatment indicated, along with immobilisation and initial avoidance of weight-bearing.Through surgical treatment we seek to achieve two objectives: optimal anatomical reduction, a factor that directly influences the results; and the stability of the first, second and third cuneiform-metatarsal joints.There are three main controversies regarding the surgical treatment of Lisfranc injuries: osteosynthesis versus primary arthrodesis; transarticular screws versus dorsal plates; and the most appropriate surgical approach.The surgical treatment we prefer is open reduction and internal fixation (ORIF) with transarticular screws or with dorsal plates in cases of comminution of metatarsals or cuneiform bones. Cite this article: EFORT Open Rev 2019;4:430-444. DOI: 10.1302/2058-5241.4.180076.
Keywords: Lisfranc fracture-dislocation; Lisfranc joint; diagnosis; results; tarsometatarsal joint; treatment.
Conflict of interest statement
ICMJE Conflict of interest statement: The author declares no conflict of interest relevant to this work.
Figures




References
-
- Cassebaum WH. Lisfranc fracture-dislocations. Clin Orthop Relat Res 1963;30(30):116–129. - PubMed
-
- Desmond EA, Chou LB. Current concepts review: Lisfranc injuries. Foot Ankle Int 2006;27(8):653–660. - PubMed
-
- Myerson MS, Cerrato R. Current management of tarsometatarsal injuries in the athlete. Instr Course Lect 2009;58:583–594. - PubMed
-
- Benirschke SK, Meinberg E, Anderson SA, Jones CB, Cole PA. Fractures and dislocations of the midfoot: Lisfranc and Chopart injuries. J Bone Joint Surg [Am] 2012;94(14):1325–1337. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
