

Systemic Inflammation Rapidly Induces Reversible Atrial Electrical Remodeling: The Role of Interleukin-6-Mediated Changes in Connexin Expression
- PMID: 31423933
- PMCID: PMC6759884
- DOI: 10.1161/JAHA.118.011006
Systemic Inflammation Rapidly Induces Reversible Atrial Electrical Remodeling: The Role of Interleukin-6-Mediated Changes in Connexin Expression
Abstract
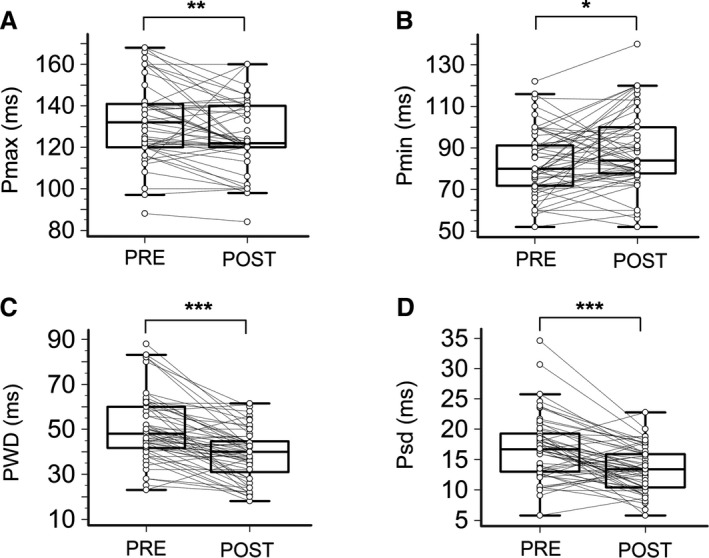
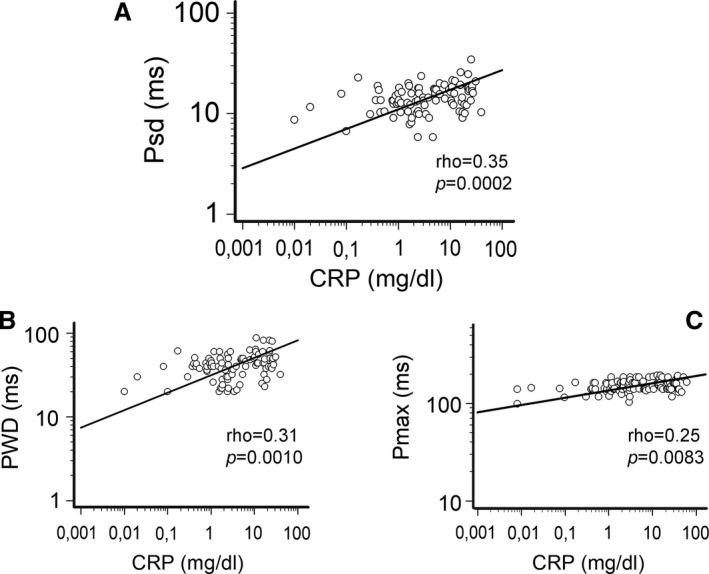
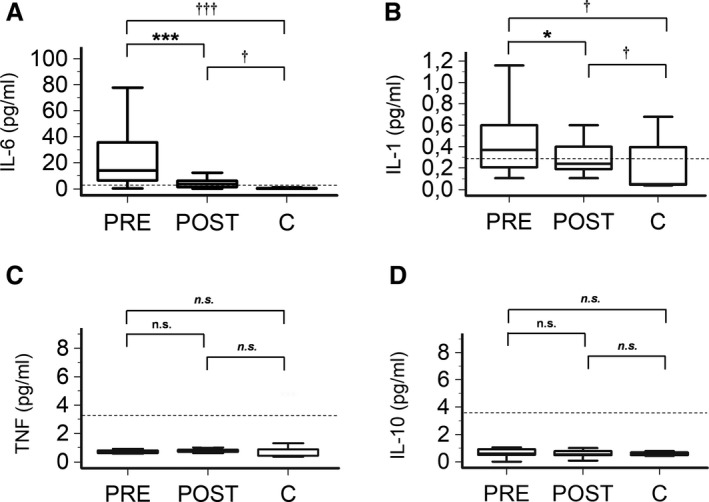
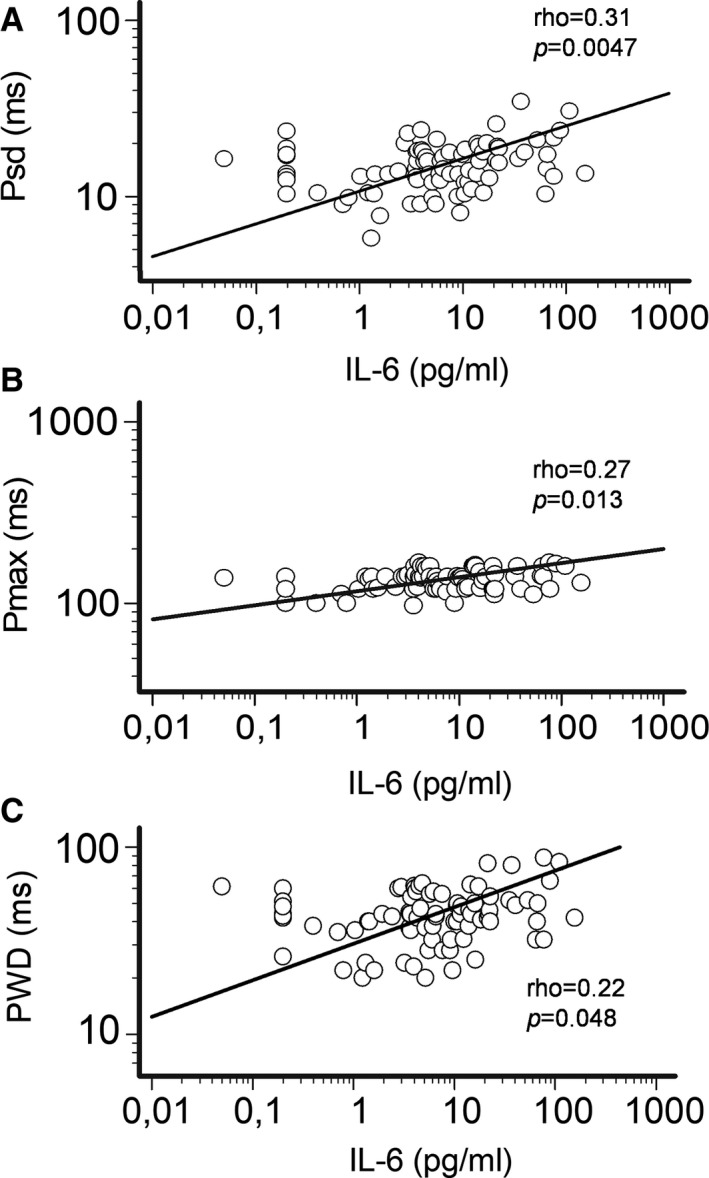
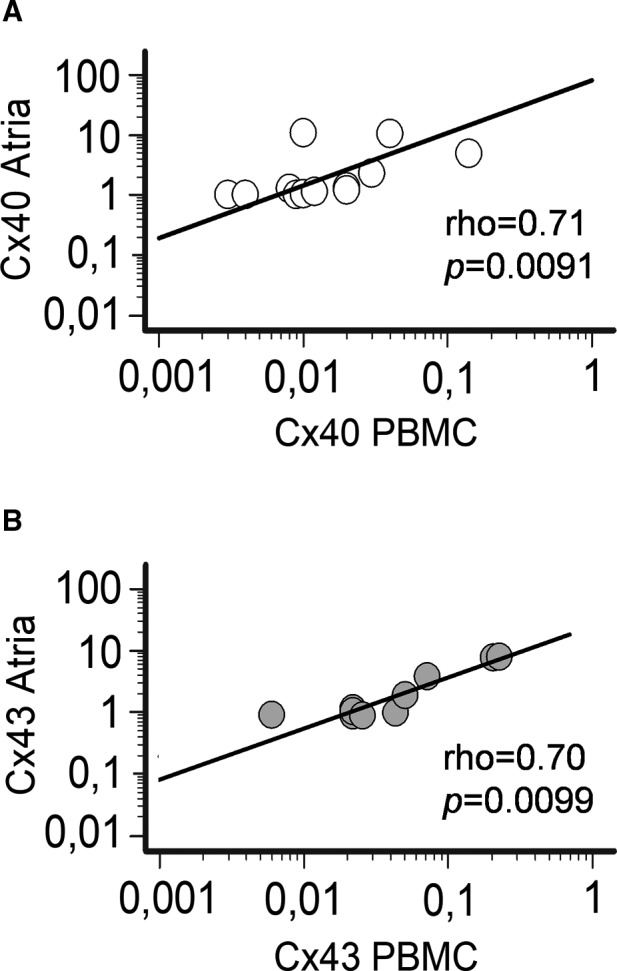
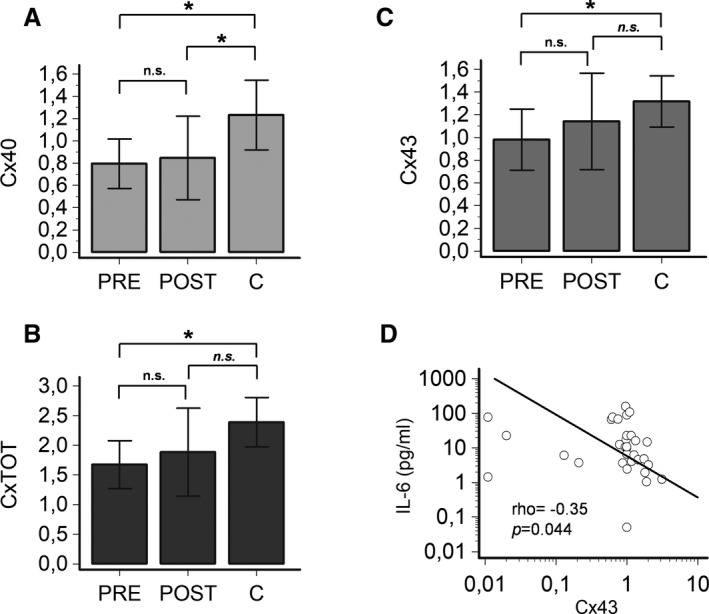
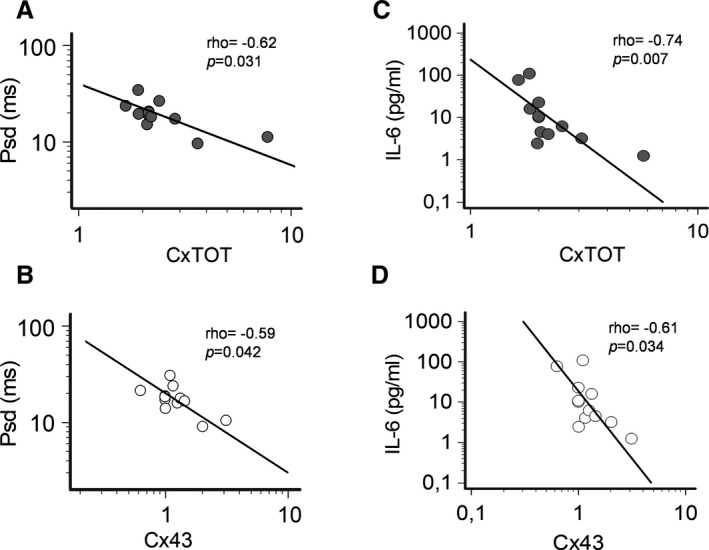
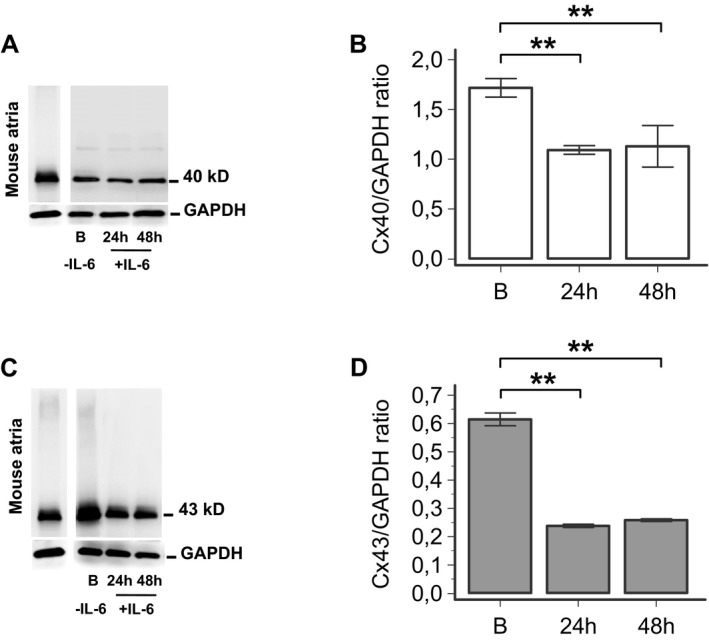
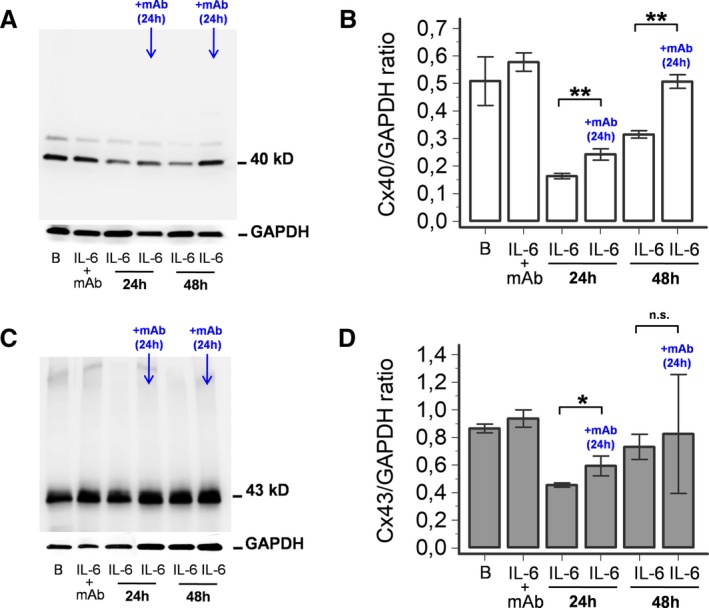
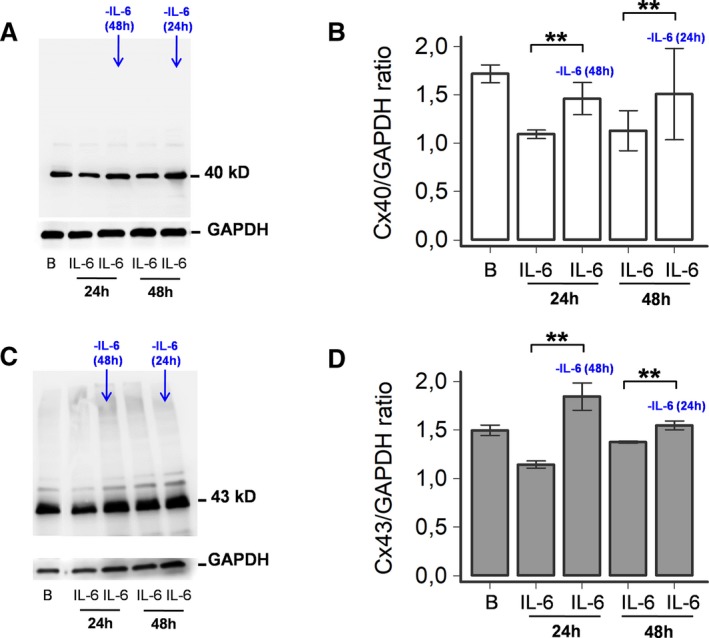
Background Systemic inflammation is a strong predictor of atrial fibrillation. A key role for electrical remodeling is increasingly recognized, and experimental data suggest that inflammatory cytokines can directly affect connexins resulting in gap-junction dysfunction. We hypothesized that systemic inflammation, regardless of its origin, promotes atrial electric remodeling in vivo, as a result of cytokine-mediated changes in connexin expression. Methods and Results Fifty-four patients with different inflammatory diseases and elevated C-reactive protein were prospectively enrolled, and electrocardiographic P-wave dispersion indices, cytokine levels (interleukin-6, tumor necrosis factor-α, interleukin-1, interleukin-10), and connexin expression (connexin 40, connexin 43) were measured during active disease and after reducing C-reactive protein by >75%. Moreover, peripheral blood mononuclear cells and atrial tissue specimens from an additional sample of 12 patients undergoing cardiac surgery were evaluated for atrial and circulating mRNA levels of connexins. Finally, in vitro effects of interleukin-6 on connexin expression were studied in HL-1 mouse atrial myocytes. In patients with active inflammatory diseases, P-wave dispersion indices were increased but rapidly decreased within days when C-reactive protein normalizes and interleukin-6 levels decline. In inflammatory disease patients, both P-wave dispersion indices and interleukin-6 changes were inversely associated with circulating connexin levels, and a positive correlation between connexin expression in peripheral blood mononuclear cells and atrial tissue was demonstrated. Moreover, interleukin-6 significantly reduced connexin expression in HL-1 cells. Conclusions Our data suggest that regardless of specific etiology and organ localization, systemic inflammation, via interleukin-6 elevation, rapidly induces atrial electrical remodeling by down-regulating cardiac connexins. Although transient, these changes may significantly increase the risk for atrial fibrillation and related complications during active inflammatory processes.
Keywords: P‐wave indices; atrial electrical remodeling; atrial fibrillation; connexins; interleukin‐6; systemic inflammation.
Figures
Comment in
-
IL-6 Rapidly Induces Reversible Atrial Electrical Remodeling by Downregulation of Cardiac Connexins.J Am Heart Assoc. 2019 Aug 20;8(16):e013638. doi: 10.1161/JAHA.119.013638. Epub 2019 Aug 19. J Am Heart Assoc. 2019. PMID: 31423871 Free PMC article.
References
-
- Dobrev D, Nattel S. New antiarrhythmic drugs for treatment of atrial fibrillation. Lancet. 2010;1212–1223. - PubMed
-
- Kato T, Iwasaki YK, Nattel S. Connexins and atrial fibrillation: filling in the gaps. Circulation. 2012;203–206. - PubMed
-
- Hu YF, Chen YJ, Lin YJ, Chen SA. Inflammation and the pathogenesis of atrial fibrillation. Nat Rev Cardiol. 2015;230–243. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
