

Clinical significance of the bronchodilator response in children with severe asthma
- PMID: 31424170
- PMCID: PMC7015037
- DOI: 10.1002/ppul.24473
Clinical significance of the bronchodilator response in children with severe asthma
Abstract
Background: Our objective was to determine those characteristics associated with reversibility of airflow obstruction and response to maximal bronchodilation in children with severe asthma through the Severe Asthma Research Program (SARP).
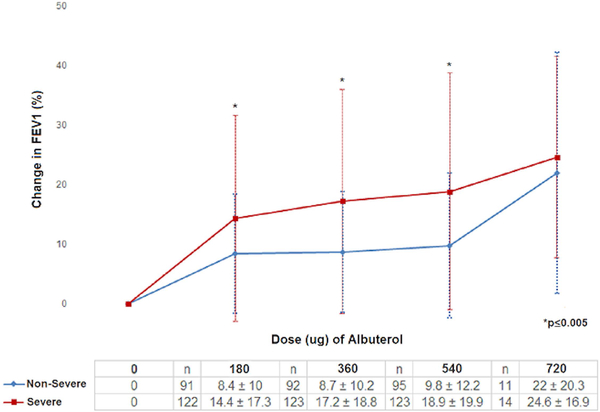
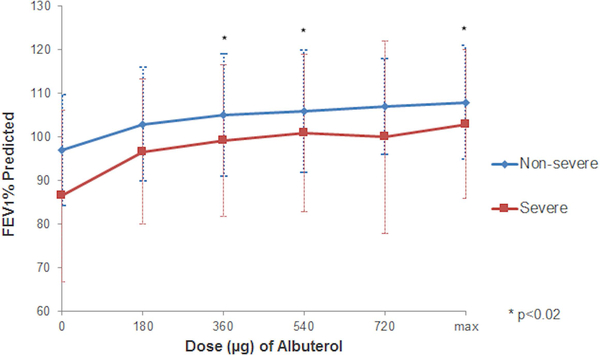
Methods: We performed a cross-sectional analysis evaluating children ages 6 to 17 years with nonsevere asthma (NSA) and severe asthma (SA). Participants underwent spirometry before and after 180 µg of albuterol to determine reversibility (≥12% increase in FEV1 ). Participants were then given escalating doses up to 720 µg of albuterol to determine their maximum reversibility.
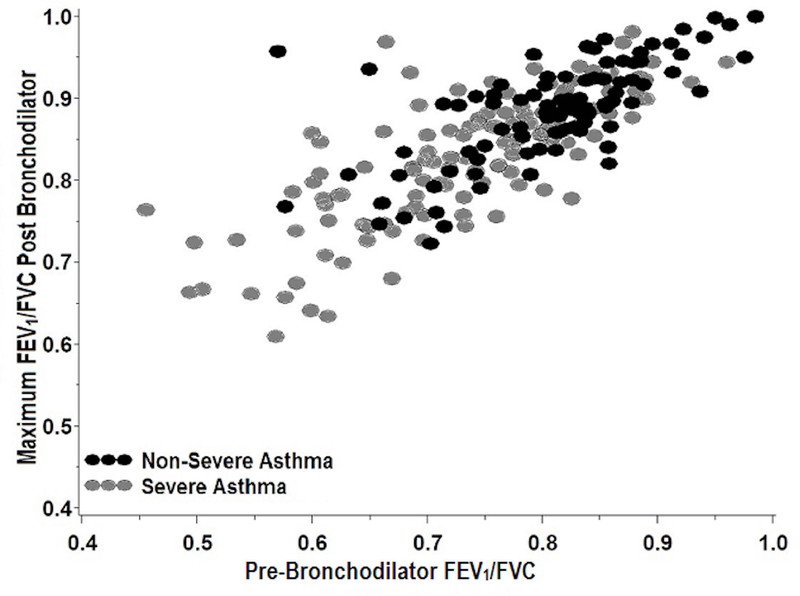
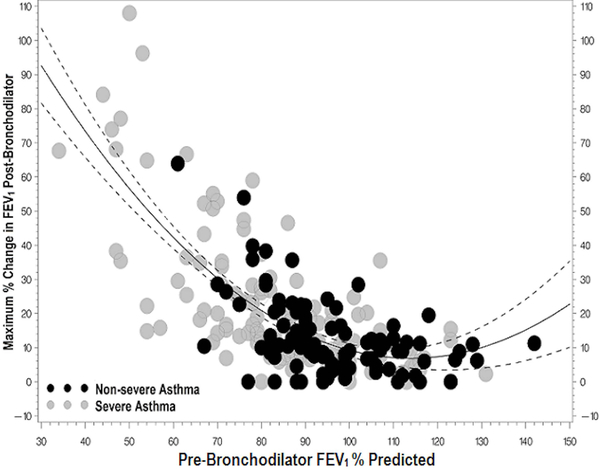
Results: We evaluated 230 children (n = 129 SA, n = 101 NSA) from five centers across the United States in the SARP I and II cohorts. SA (odds ratio [OR], 2.08, 95% confidence interval [CI], 1.05-4.13), second-hand smoke exposure (OR, 2.81, 95%CI, 1.23-6.43), and fractional exhaled nitric oxide (FeNO; OR, 1.97, 95%CI, 1.35-2.87) were associated with increased odds of airway reversibility after maximal bronchodilation, while higher prebronchodilator (BD) FEV1 % predicted (OR, 0.91, 95%CI, 0.88-0.94) was associated with decreased odds. In an analysis using the SARP III cohort (n = 186), blood neutrophils, immunoglobulin E (IgE), and FEV1 % predicted were significantly associated with BD reversibility. In addition, children with BD response have greater healthcare utilization. BD reversibility was associated with reduced lung function at enrollment and 1-year follow-up though less decline in lung function over 1 year compared to those without reversibility.
Conclusions: Lung function, that is FEV1 % predicted, is a predictor of BD response in children with asthma. Additionally, smoke exposure, higher FeNO or IgE level, and low peripheral blood neutrophils are associated with a greater likelihood of BD reversibility. BD response can identify a phenotype of pediatric asthma associated with low lung function and poor asthma control.
Keywords: asthma; bronchodilator response; pediatrics.
© 2019 Wiley Periodicals, Inc.
Figures

References
-
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson P, Hankinson J. et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948–68. - PubMed
-
- Proceedings of the ATS workshop on refractory asthma: current understanding, recommendations, and unanswered questions. American Thoracic Society. Am J Respir Crit Care Med 2000;162:2341–51. - PubMed
-
- Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, Adcock IM, Bateman ED, Bel EH, Bleecker ER, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J 2014;43:343–73. - PubMed
