

A Collimator Setting Optimization Algorithm for Dual-Arc Volumetric Modulated Arc Therapy in Pancreas Stereotactic Body Radiation Therapy
- PMID: 31426721
- PMCID: PMC6702773
- DOI: 10.1177/1533033819870767
A Collimator Setting Optimization Algorithm for Dual-Arc Volumetric Modulated Arc Therapy in Pancreas Stereotactic Body Radiation Therapy
Abstract
Purpose: To optimize collimator setting to improve dosimetric quality of pancreas volumetric modulated arc therapy plan for stereotactic body radiation therapy.
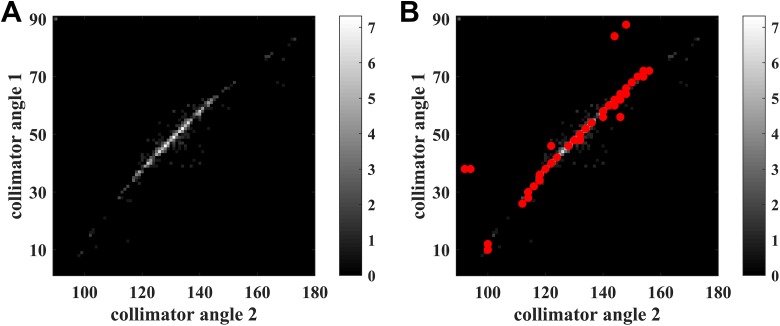
Materials and methods: Fifty-five volumetric modulated arc therapy cases in stereotactic body radiation therapy of pancreas were retrospectively included in this study with internal review board approval. Different from the routine practice of initializing collimator settings with a template, the proposed algorithm simultaneously optimizes the collimator angles and jaw positions that are customized to the patient geometry. Specifically, this algorithm includes 2 key steps: (1) an iterative optimization algorithm via simulated annealing that generates a set of potential collimator settings from 39 cases with pancreas stereotactic body radiation therapy, and (2) a multi-leaf collimator modulation scoring system that makes the final decision of the optimal collimator settings (collimator angles and jaw positions) based on organs at risk sparing criteria. For validation, the other 16 cases with pancreas stereotactic body radiation therapy were analyzed. Two plans were generated for each validation case, with one plan optimized using the proposed algorithm (Planopt) and the other plan with the template setting (Planconv). Each plan was optimized with 2 full arcs and the same set of constraints for the same case. Dosimetric results were analyzed and compared, including target dose coverage, conformity, organs at risk maximum dose, and modulation complexity score. All results were tested by Wilcoxon signed rank tests, and the statistical significance level was set to .05.
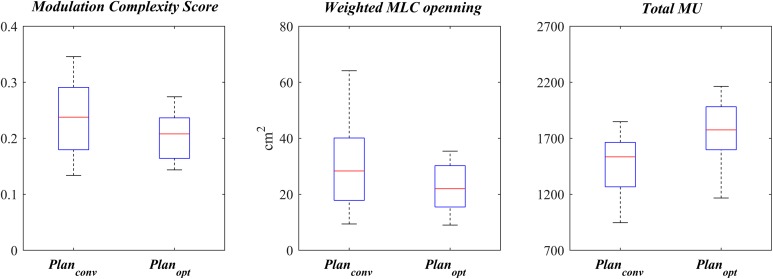
Results: Both plan groups had comparable target dose coverage and mean doses of all organs at risk. However, organs at risk (stomach, duodenum, large/small bowel) maximum dose sparing (D0.1 cc and D0.03 cc) was improved in Planopt compared to Planconv. Planopt also showed lower modulation complexity score, which suggests better capability of handling complex shape and sparing organs at risk .
Conclusions: The proposed collimator settings optimization algorithm successfully improved dosimetric performance for dual-arc pancreas volumetric modulated arc therapy plans in stereotactic body radiation therapy of pancreas. This algorithm has the capability of immediate clinical application.
Keywords: IMRT; SBRT; VMAT; collimator settings; optimization; pancreas cancer; simulated annealing; treatment planning.
Conflict of interest statement
Figures




References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics 2018. CA Cancer J Clini. 2018;68(1):7–30. - PubMed
-
- Tempero MA, Malafa MP, Al-Hawary M. et al. Pancreatic adenocarcinoma: clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2010;8(9):1028–1061. - PubMed
-
- Simianu VV, Zyromski NJ, Nakeeb A, Lillemoe KD. Pancreatic cancer: progress made. Acta Oncol. 2010:49(4):407–417. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
