

Update on lactose malabsorption and intolerance: pathogenesis, diagnosis and clinical management
- PMID: 31427404
- PMCID: PMC6839734
- DOI: 10.1136/gutjnl-2019-318404
Update on lactose malabsorption and intolerance: pathogenesis, diagnosis and clinical management
Abstract
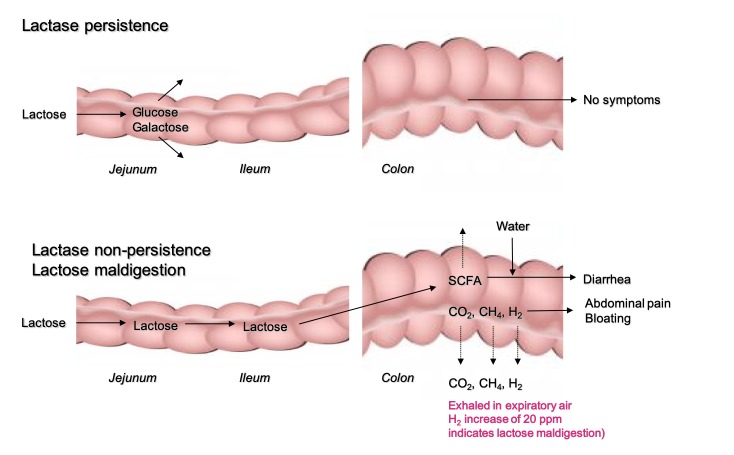
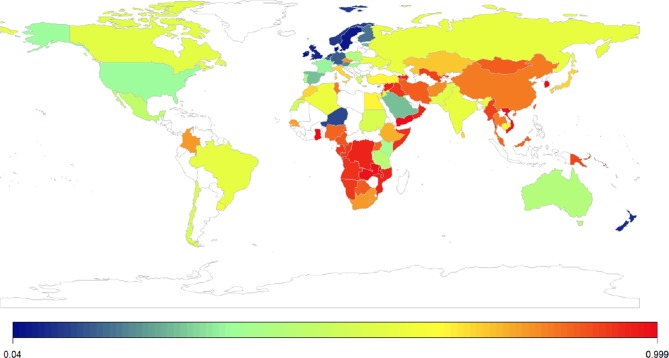
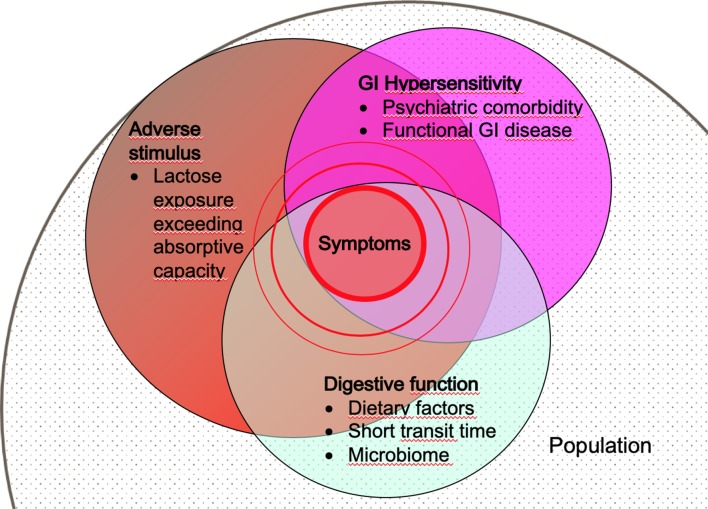
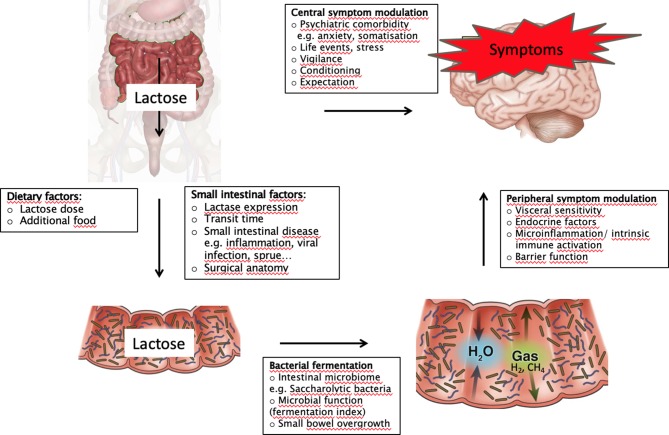
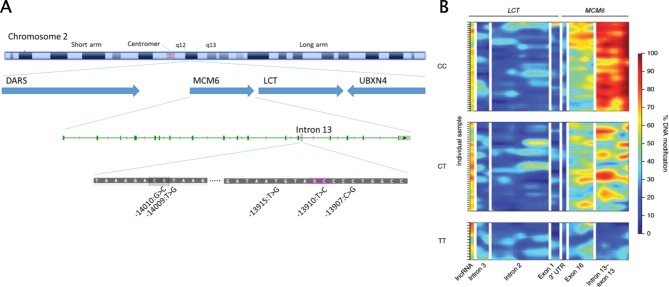
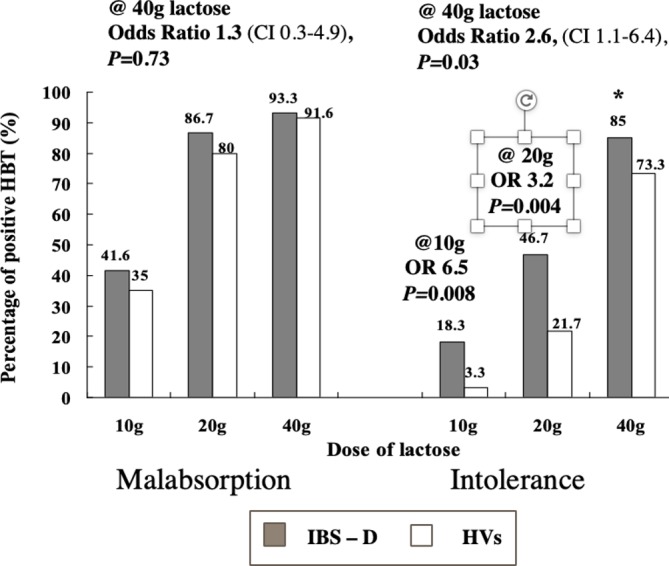
Lactose is the main source of calories in milk, an essential nutriedigestion, patients with visceral hypersensitivity nt in infancy and a key part of the diet in populations that maintain the ability to digest this disaccharide in adulthood. Lactase deficiency (LD) is the failure to express the enzyme that hydrolyses lactose into galactose and glucose in the small intestine. The genetic mechanism of lactase persistence in adult Caucasians is mediated by a single C→T nucleotide polymorphism at the LCTbo -13'910 locus on chromosome-2. Lactose malabsorption (LM) refers to any cause of failure to digest and/or absorb lactose in the small intestine. This includes primary genetic and also secondary LD due to infection or other conditions that affect the mucosal integrity of the small bowel. Lactose intolerance (LI) is defined as the onset of abdominal symptoms such as abdominal pain, bloating and diarrhoea after lactose ingestion by an individual with LM. The likelihood of LI depends on the lactose dose, lactase expression and the intestinal microbiome. Independent of lactose digestion, patients with visceral hypersensitivity associated with anxiety or the Irritable Bowel Syndrome (IBS) are at increased risk of the condition. Diagnostic investigations available to diagnose LM and LI include genetic, endoscopic and physiological tests. The association between self-reported LI, objective findings and clinical outcome of dietary intervention is variable. Treatment of LI can include low-lactose diet, lactase supplementation and, potentially, colonic adaptation by prebiotics. The clinical outcome of these treatments is modest, because lactose is just one of a number of poorly absorbed carbohydrates which can cause symptoms by similar mechanisms.
Keywords: diet; functional bowel disorder; hydrogen breath tests; lactase; malabsorption.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MF has received research funding from Nestlé International for studies of lactose digestion and tolerance.
Figures
Comment in
-
Role of the gut microbiome in mediating lactose intolerance symptoms.Gut. 2022 Jan;71(1):215-217. doi: 10.1136/gutjnl-2020-323911. Epub 2021 Mar 18. Gut. 2022. PMID: 34086598 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials