

A Rare Case of Steroid Cell Tumor, Not Otherwise Specified (NOS), of the Ovary in a Young Woman
- PMID: 31428489
- PMCID: PMC6683816
- DOI: 10.1155/2019/4375839
A Rare Case of Steroid Cell Tumor, Not Otherwise Specified (NOS), of the Ovary in a Young Woman
Abstract
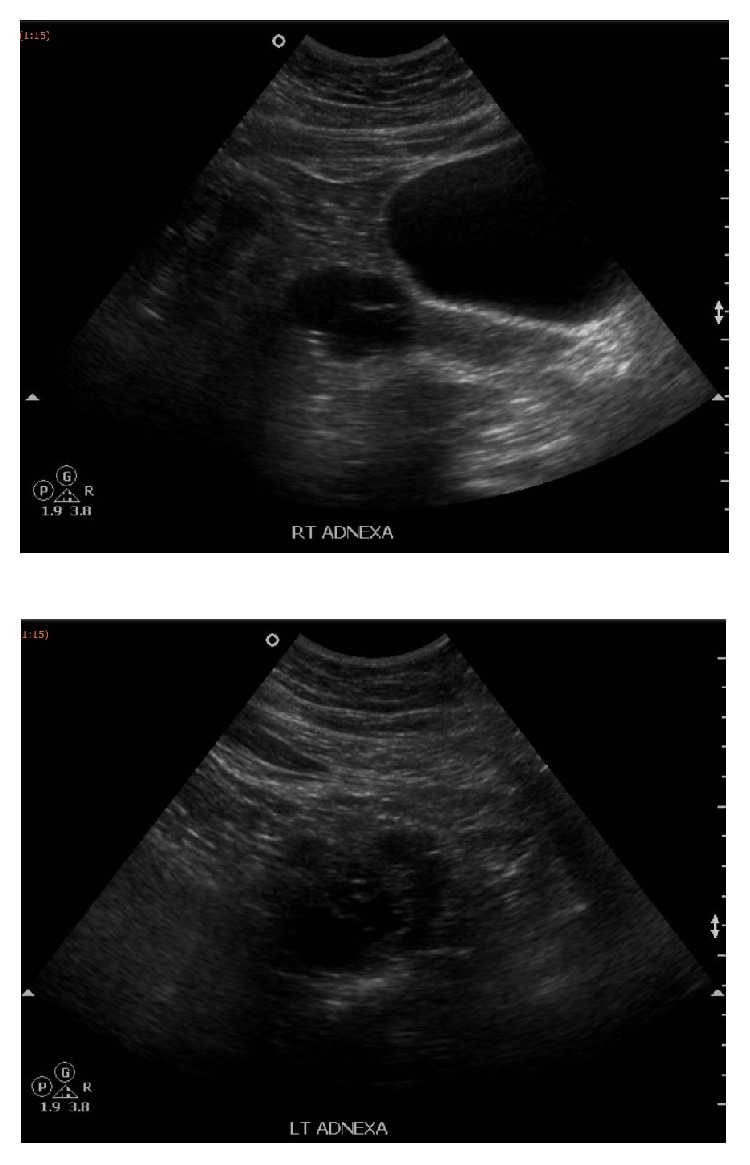
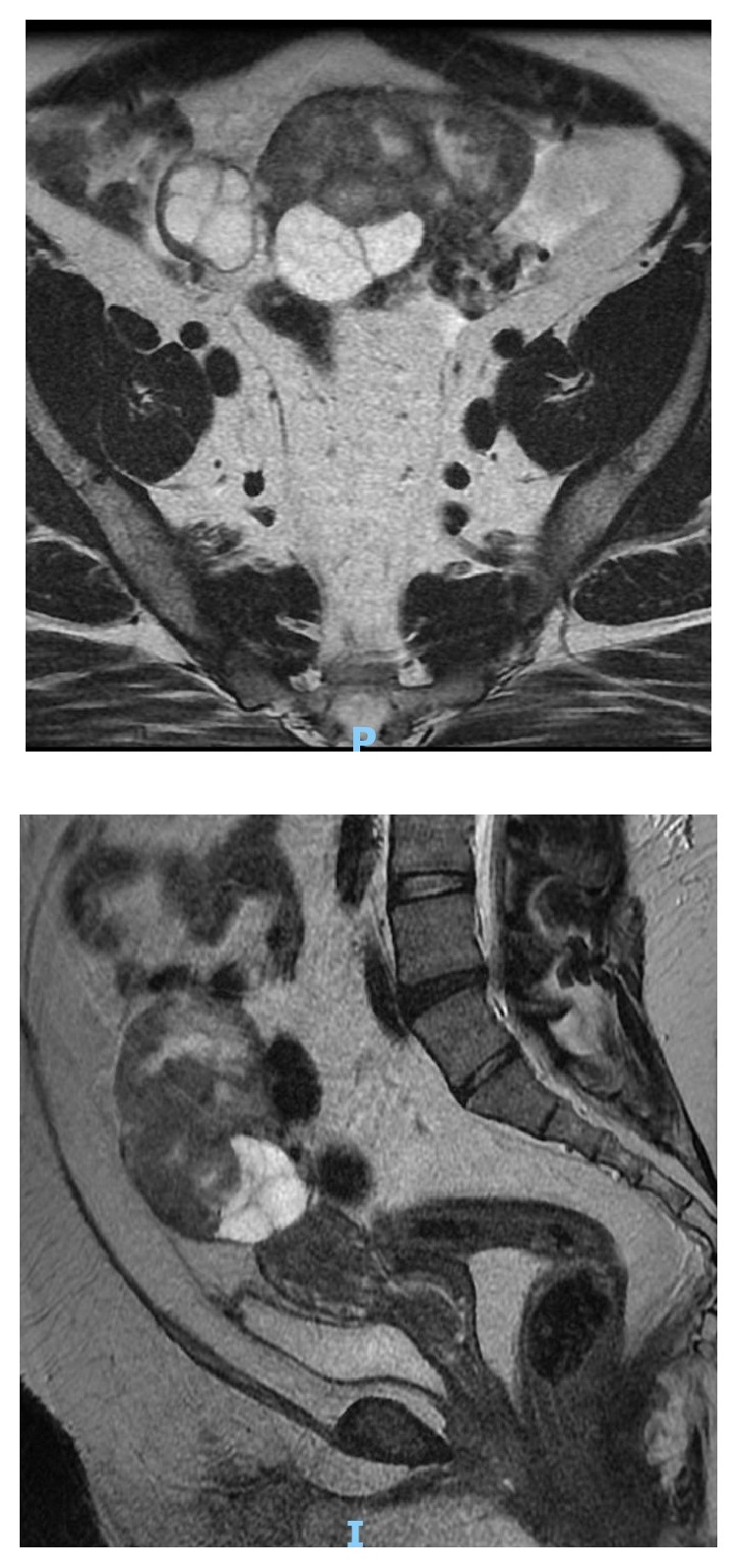
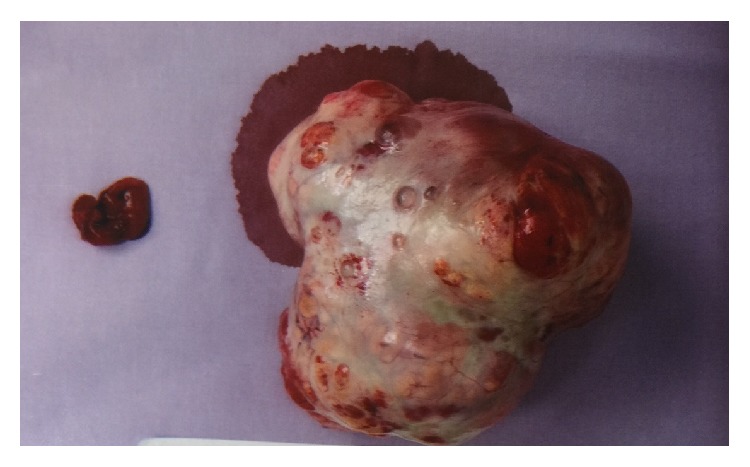
Steroid cell tumour is a rare sex cord-stromal tumor of the ovary. It may produce steroids and is associated with testosterone secretion which causes symptoms like hair loss, hirsutism, and oligomenorrhea/amenorrhea due to hormonal activity and virilizing properties of tumor. In this article, we reported a 27-year-old woman who presented with hirsutism, hoarseness of voice, scalp hair fall, and amenorrhea for 8 years. Clinical and diagnostic evaluation revealed a left adnexal mass and elevated serum levels of testosterone and she was diagnosed as having a Sertoli Leydig cell tumour of ovary. She underwent left salpingooophorectomy and both histopathological examination and immunohistochemistry confirmed the diagnosis. Her serum testosterone levels normalized 3 days after the surgery and her menses resumed spontaneously a few months after the operation. In addition, we reviewed the literature on the epidemiology, clinical presentations, imaging and histological findings, and the treatment options on this disease.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Young R. H., Clement P. B., Scully R. E. Sex-cord, stromal, steroid cell and germ cell tumours of the ovary. In: Mills S.-E., Carter D., Greenson J.-K., Oberman H.-A., Reuter V., Stoler M.-H., editors. Sternbergs Diagnostic Surgical Pathology. 4. Philadelphia, Pa, USA: Lippincott Williams & Wilkins; 2004. pp. 2579–2615.
-
- Revathy M., Kanchana M. P. Incidence of virilisation in sex cord stromal tumours of ovary, a 5-year experience in a tertiary care gynaecological centre. Journal of Evolution of Medical and Dental Sciences. 2018;7(7):886–891. doi: 10.14260/jemds/2018/202. - DOI
-
- Seles F. M., Revathy M., Kanchana M. P. Steroid cell tumour of the ovary: a case report with review of literature. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2018;7:3425–3428.
Publication types
LinkOut - more resources
Full Text Sources
