

Magnetic resonance imaging of the papillary muscles of the left ventricle: normal anatomy, variants, and abnormalities
- PMID: 31428880
- PMCID: PMC6702502
- DOI: 10.1186/s13244-019-0761-3
Magnetic resonance imaging of the papillary muscles of the left ventricle: normal anatomy, variants, and abnormalities
Abstract
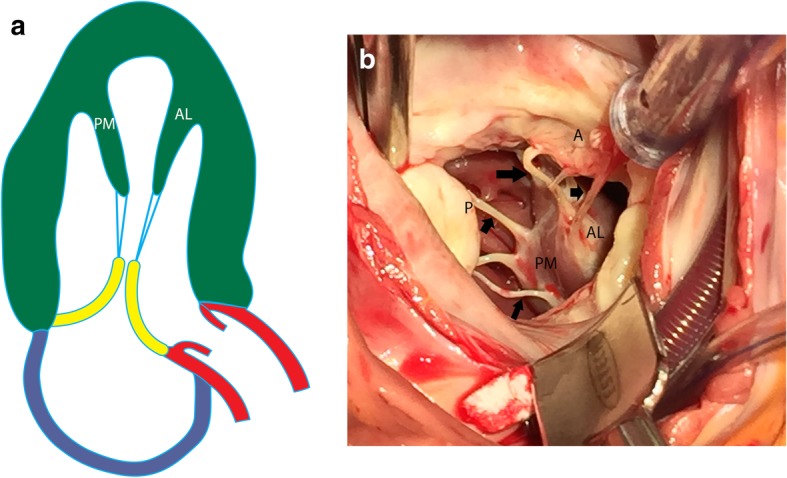
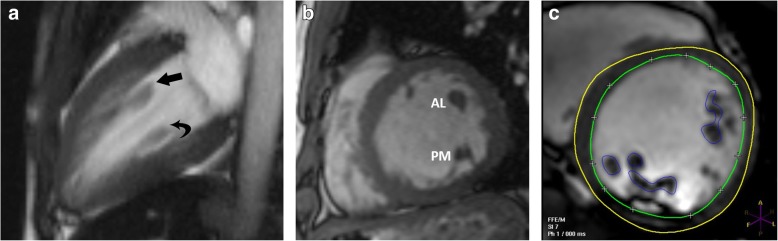
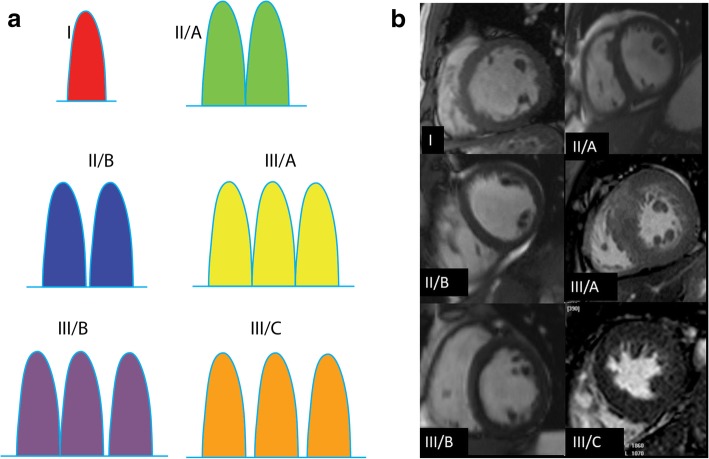
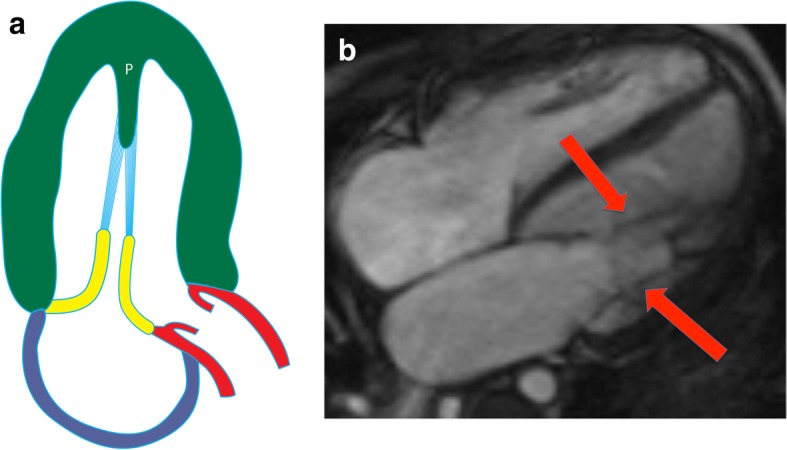
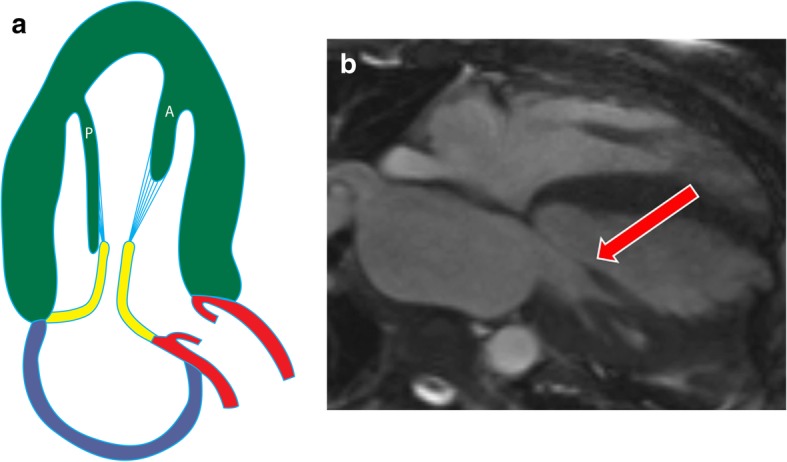
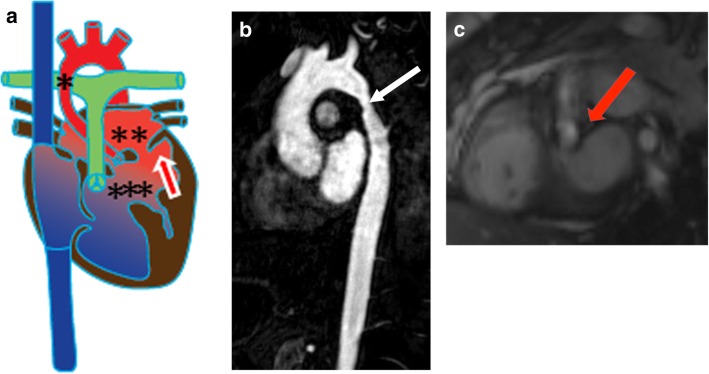
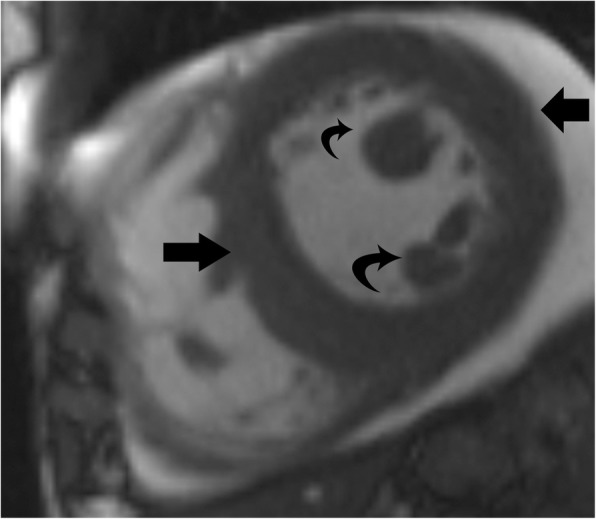
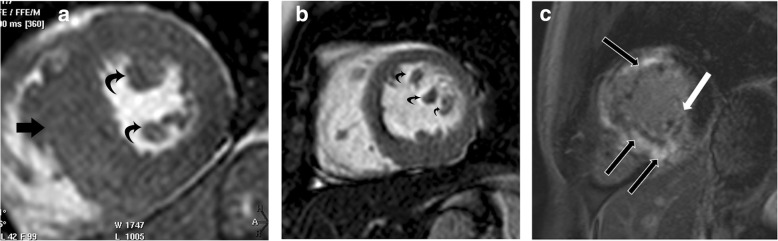
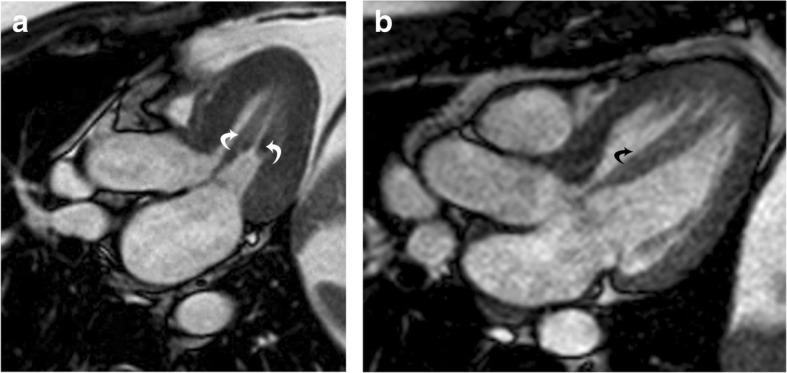
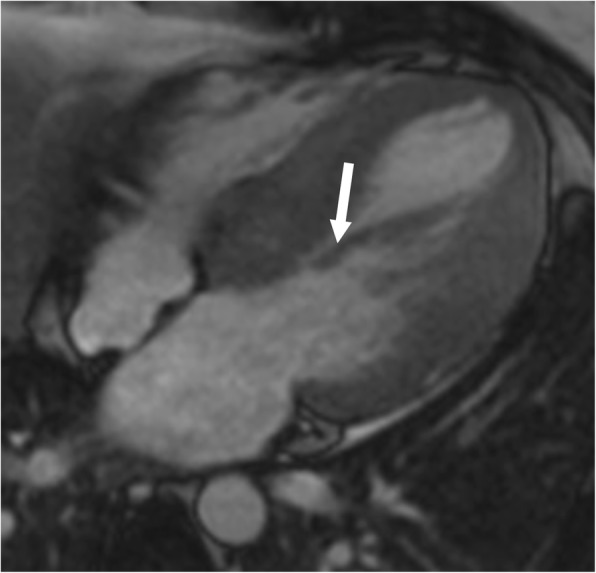
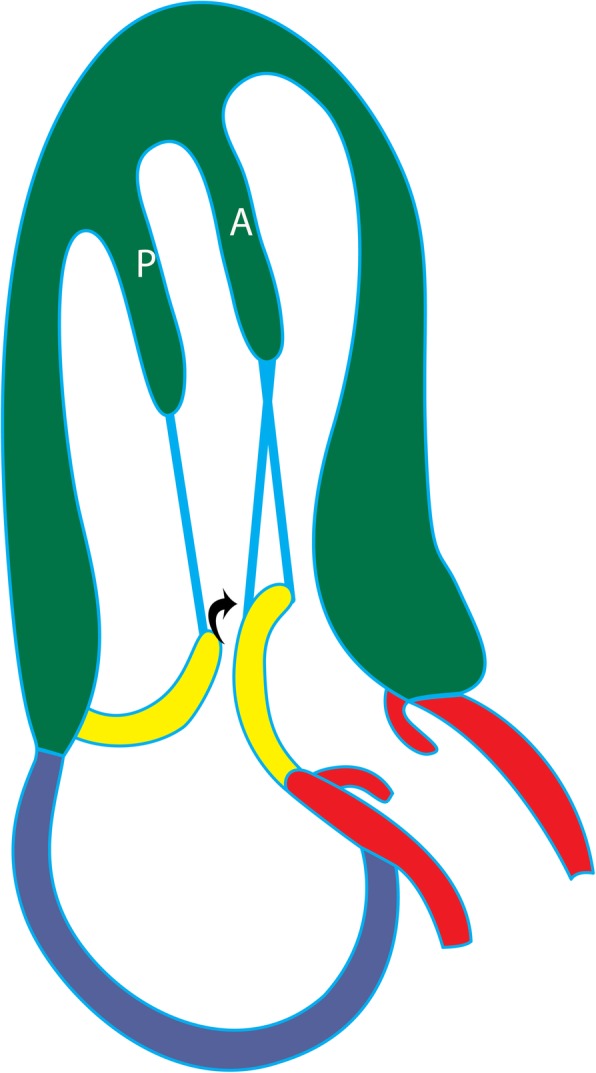
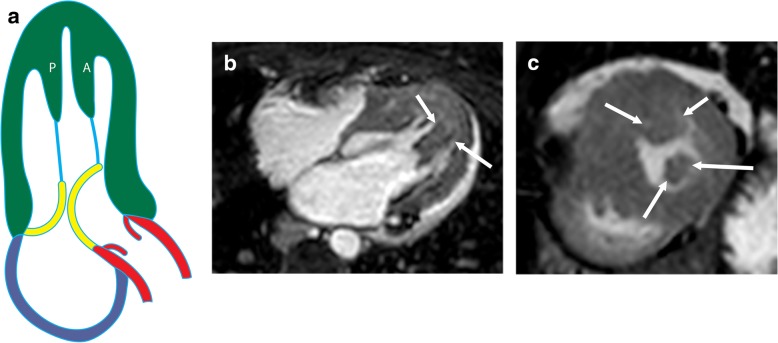
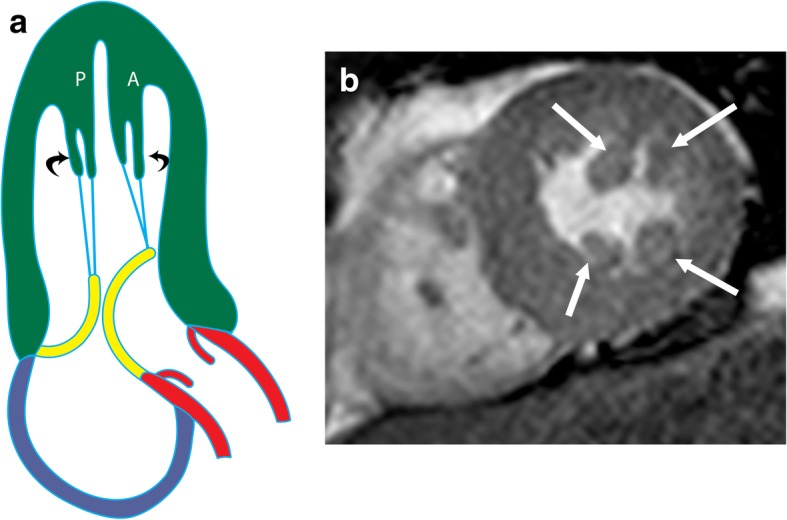
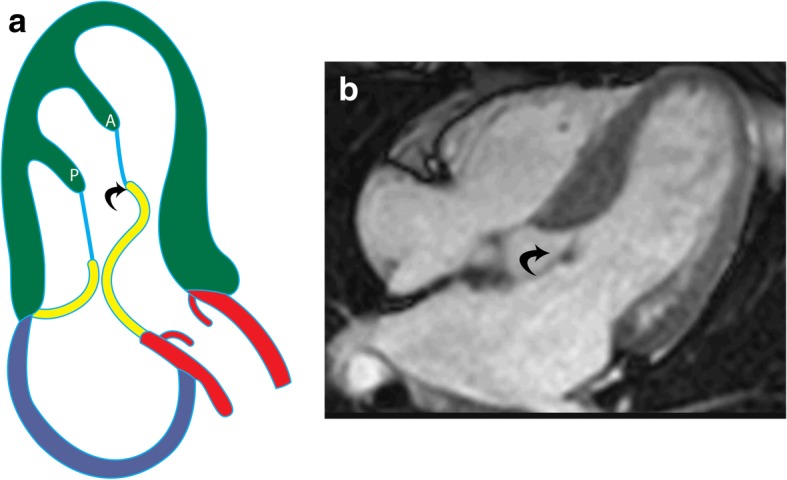
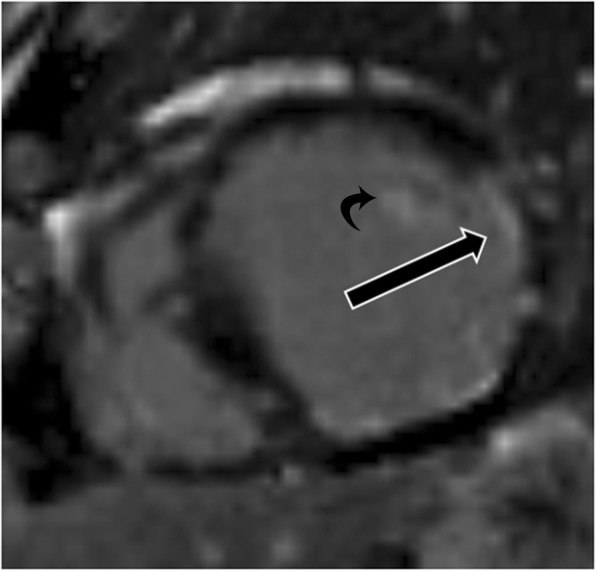
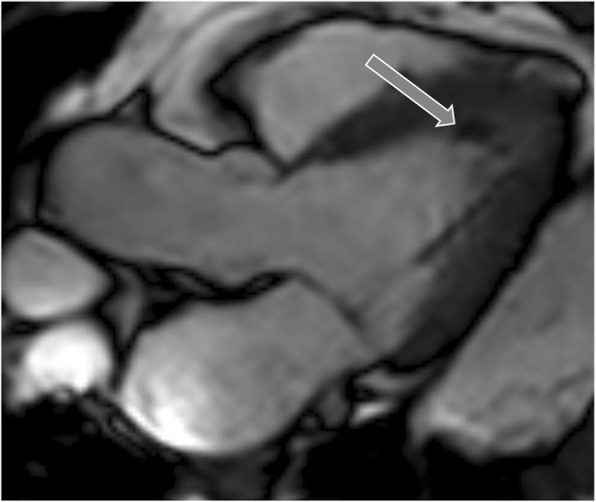
Left ventricular papillary muscles are small myocardial structures that play an important role in the functioning of mitral valve and left ventricle. Typically, there are two groups of papillary muscles, namely the anterolateral and the posteromedial groups. Cardiovascular magnetic resonance (CMR) is a valuable imaging modality in the evaluation of papillary muscles, providing both morphological and functional information. There is a remarkably wide variation in the morphology of papillary muscles. These variations can be asymptomatic or associated with symptoms related to LV outflow tract obstruction, often associated with hypertrophic cardiomyopathy. Abnormalities of the papillary muscles range from congenital disorders to neoplasms. Parachute mitral valve is the most common congenital abnormality of papillary muscles, in which all the chordae insert into a single papillary muscle. Papillary muscles can become dysfunctional, most commonly due to ischemia. Papillary muscle rupture is a major complication of acute myocardial infarction that results in mitral regurgitation and associated with high mortality rates. The most common papillary neoplasm is metastasis, but primary benign and malignant neoplasms can also be seen. In this article, we discuss the role of CMR in the evaluation of papillary muscle anatomy, function, and abnormalities.
Keywords: Anatomy; CMR; Hypertrophic cardiomyopathy; Papillary muscles; Variants.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
