

HIV-Related Cerebral Toxoplasmosis Revisited: Current Concepts and Controversies of an Old Disease
- PMID: 31429353
- PMCID: PMC6900575
- DOI: 10.1177/2325958219867315
HIV-Related Cerebral Toxoplasmosis Revisited: Current Concepts and Controversies of an Old Disease
Abstract
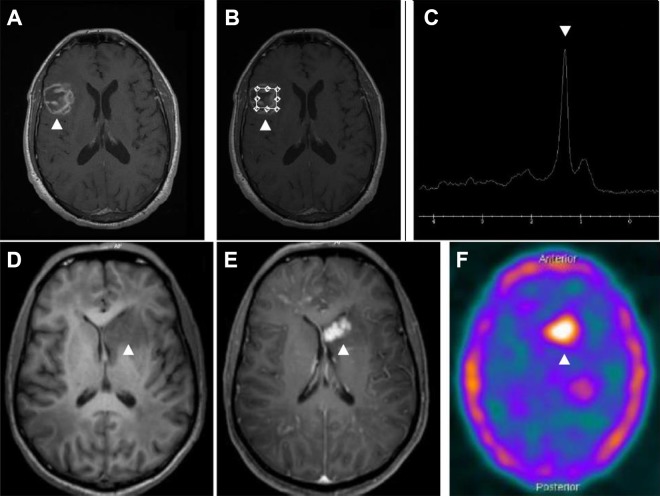
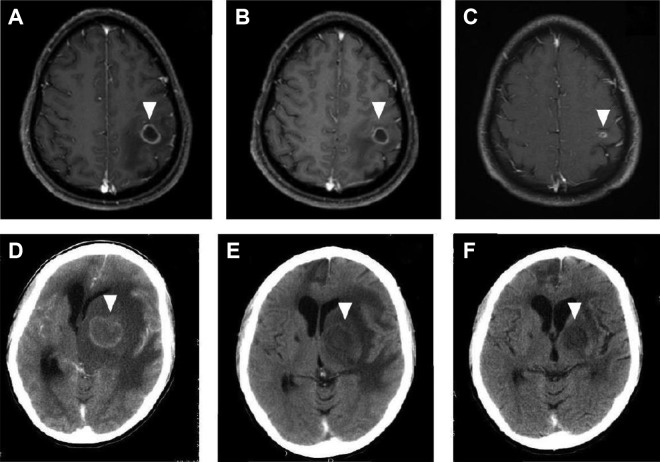
Cerebral toxoplasmosis is the most common cause of expansive brain lesions in people living with HIV/AIDS (PLWHA) and continues to cause high morbidity and mortality. The most frequent characteristics are focal subacute neurological deficits and ring-enhancing brain lesions in the basal ganglia, but the spectrum of clinical and neuroradiological manifestations is broad. Early initiation of antitoxoplasma therapy is an important feature of the diagnostic approach of expansive brain lesions in PLWHA. Pyrimethamine-based regimens and trimethoprim-sulfamethoxazole (TMP-SMX) seem to present similar efficacy, but TMP-SMX shows potential practical advantages. The immune reconstitution inflammatory syndrome is uncommon in cerebral toxoplasmosis, and we now have more effective, safe, and friendly combined antiretroviral therapy (cART) options. As a consequence of these 2 variables, the initiation of cART can be performed within 2 weeks after initiation of antitoxoplasma therapy. Herein, we will review historical and current concepts of epidemiology, diagnosis, and treatment of HIV-related cerebral toxoplasmosis.
Keywords: acquired immunodeficiency syndrome; central nervous system; cerebral toxoplasmosis; toxoplasmic encephalitis; toxoplasmosis.
Conflict of interest statement
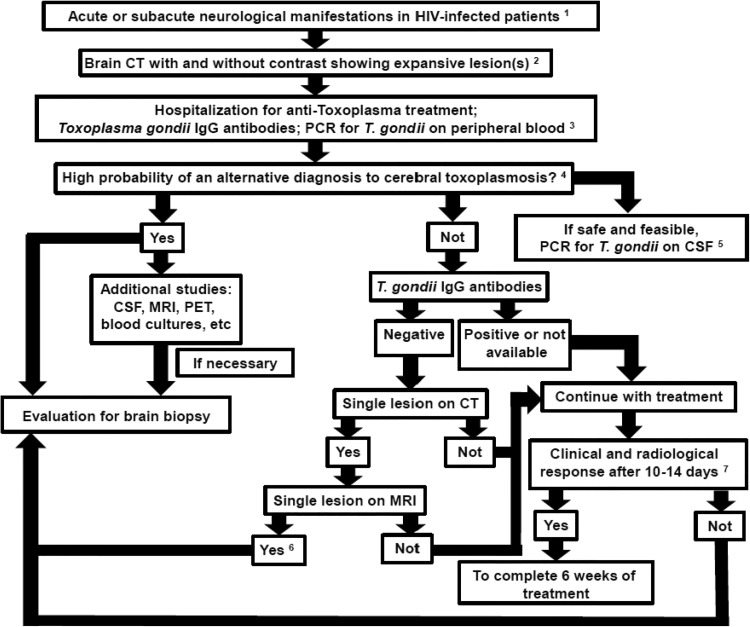
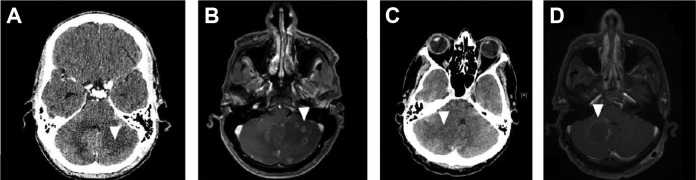
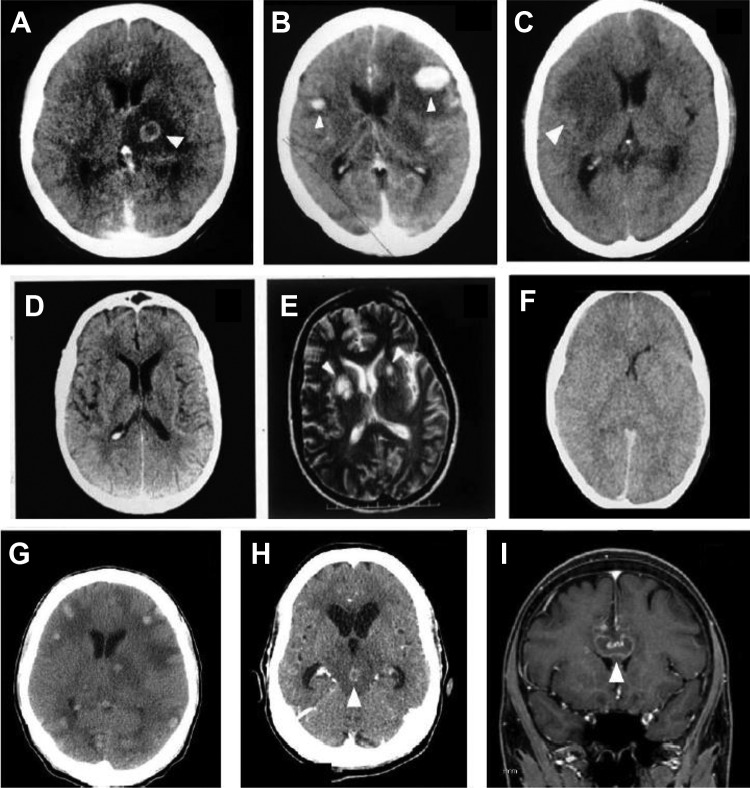
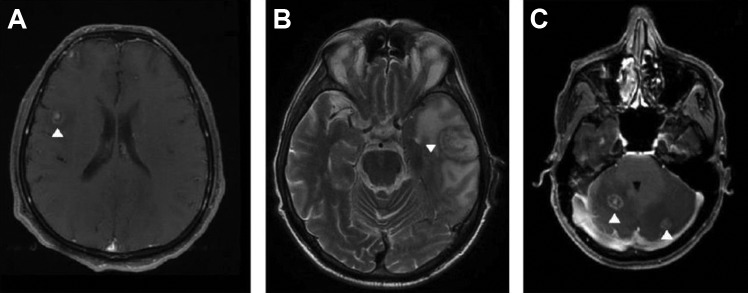
Figures
References
-
- Lyons RE, McLeod R, Roberts CW. Toxoplasma gondii tachyzoite-bradyzoite interconversion. Trends Parasitol. 2002;18(5):198–201. - PubMed
-
- Luft BJ, Hafner R, Korzun AH. et al. Toxoplasmic encephalitis in patients with the acquired immunodeficiency syndrome. Members of the ACTG 077p/ANRS 009 Study Team. N Engl J Med. 1993;329(14):995–1000. - PubMed
-
- Vilaseca J, Arnau JM, Bacardi R, Mieras C, Serrano A, Navarro C. Kaposi’s sarcoma and Toxoplasma gondii brain abscess in a Spanish homosexual. Lancet. 1982;1(8271):572. - PubMed
-
- Centers for Disease Control (CDC). Opportunistic infections and Kaposi’s sarcoma among Haitians in the United States. MMWR Morb Mortal Wkly Rep. 1982;31(26):353–354, 360-361. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
