

Association of Diabetes Mellitus on Cardiac Remodeling, Quality of Life, and Clinical Outcomes in Heart Failure With Reduced and Preserved Ejection Fraction
- PMID: 31431116
- PMCID: PMC6755825
- DOI: 10.1161/JAHA.119.013114
Association of Diabetes Mellitus on Cardiac Remodeling, Quality of Life, and Clinical Outcomes in Heart Failure With Reduced and Preserved Ejection Fraction
Abstract
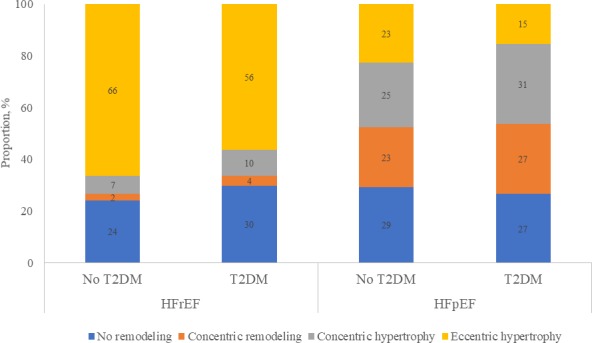
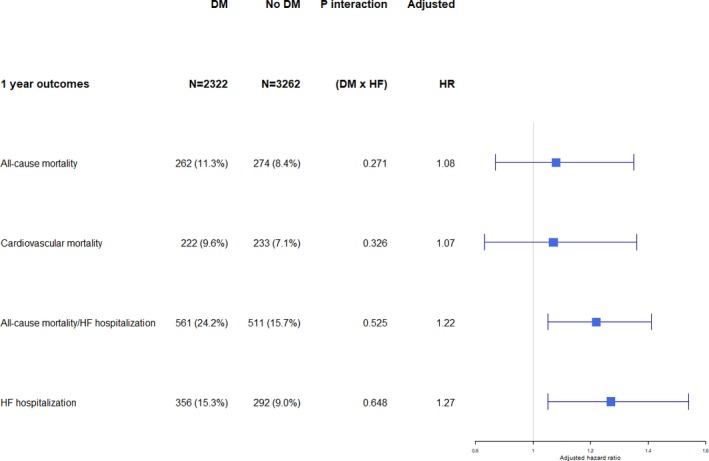
Background Diabetes mellitus frequently coexists with heart failure (HF), but few studies have compared the associations between diabetes mellitus and cardiac remodeling, quality of life, and clinical outcomes, according to HF phenotype. Methods and Results We compared echocardiographic parameters, quality of life (assessed by the Kansas City Cardiomyopathy Questionnaire), and outcomes (1-year all-cause mortality, cardiovascular mortality, and HF hospitalization) between HF patients with and without type 2 diabetes mellitus in the prospective ASIAN-HF (Asian Sudden Cardiac Death in Heart Failure) Registry, as well as community-based controls without HF. Adjusted Cox proportional hazards models were used to assess the association of diabetes mellitus with clinical outcomes. Among 5028 patients with HF and reduced ejection fraction (HFrEF; EF <40%) and 1139 patients with HF and preserved EF (HFpEF; EF ≥50%), the prevalences of type 2 diabetes mellitus were 40.2% and 45.0%, respectively (P=0.003). In both HFrEF and HFpEF cohorts, diabetes mellitus (versus no diabetes mellitus) was associated with smaller indexed left ventricular diastolic volumes and higher mitral E/e' ratio. There was a predominance of eccentric hypertrophy in HFrEF and concentric hypertrophy in HFpEF. Patients with diabetes mellitus had lower Kansas City Cardiomyopathy Questionnaire scores in both HFpEF and HFrEF, with more prominent differences in HFpEF (Pinteraction<0.05). In both HFpEF and HFrEF, patients with diabetes mellitus had more HF rehospitalizations (adjusted hazard ratio, 1.27; 95% CI, 1.05-1.54; P=0.014) and higher 1-year rates of the composite of all-cause mortality/HF hospitalization (adjusted hazard ratio, 1.22; 95% CI, 1.05-1.41; P=0.011), with no differences between HF phenotypes (Pinteraction>0.05). Conclusions In HFpEF and HFrEF, type 2 diabetes mellitus is associated with smaller left ventricular volumes, higher mitral E/e' ratio, poorer quality of life, and worse outcomes, with several differences noted between HF phenotypes. Clinical Trial Registration URL: http://www.clinicaltrials.gov. Unique identifier: NCT01633398.
Keywords: diabetes mellitus; diabetic cardiomyopathy; echocardiography; heart failure; preserved left ventricular function.
Figures
References
-
- Yoon KH, Lee JH, Kim JW, Cho JH, Choi YH, Ko SH, Zimmet P, Son HY. Epidemic obesity and type 2 diabetes in Asia. Lancet. 2006;368:1681–1688. - PubMed
-
- From AM, Leibson CL, Bursi F, Redfield MM, Weston SA, Jacobsen SJ, Rodeheffer RJ, Roger VL. Diabetes in heart failure: prevalence and impact on outcome in the population. Am J Med. 2006;119:591–599. - PubMed
-
- Bank IEM, Gijsberts CM, Teng TK, Benson L, Sim D, Yeo PSD, Ong HY, Jaufeerally F, Leong GKT, Ling LH, Richards AM, de Kleijn DPV, Dahlstrom U, Lund LH, Lam CSP. Prevalence and clinical significance of diabetes in Asian versus white patients with heart failure. JACC Heart Fail. 2017;5:14–24. - PubMed
-
- Cooper LB, Yap J, Tay WT, Teng TK, MacDonald M, Anand IS, Sharma A, O'Connor CM, Kraus WE, Mentz RJ, Lam CS. Multi‐ethnic comparisons of diabetes in heart failure with reduced ejection fraction: insights from the HF‐ACTION trial and the ASIAN‐HF registry. Eur J Heart Fail. 2018;20:1281–1289. - PubMed
-
- Seferovic PM, Paulus WJ. Clinical diabetic cardiomyopathy: a two‐faced disease with restrictive and dilated phenotypes. Eur Heart J. 2015;36:1718–1727, 1727a–1727c. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
