

The Use of Rapid Tranquilization in Aggressive Behavior
- PMID: 31431244
- PMCID: PMC6712906
- DOI: 10.3238/arztebl.2019.0445
The Use of Rapid Tranquilization in Aggressive Behavior
Abstract
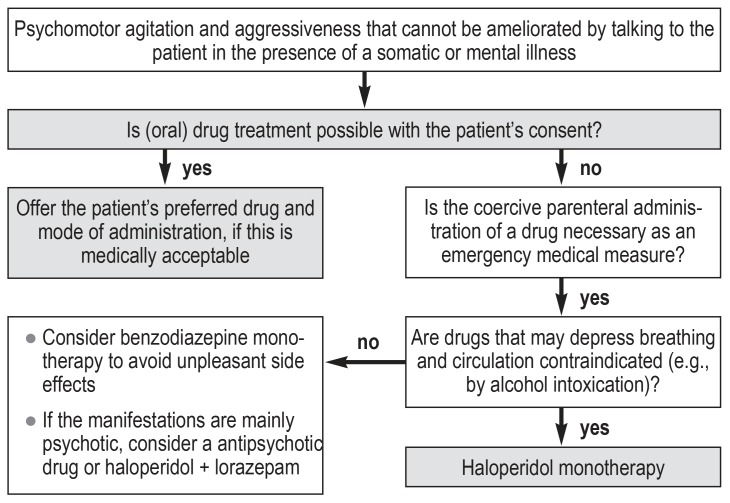
Background: Psychomotor agitation and aggressiveness in the context of mental illnessare medical emergencies. In a survey of six German psychiatric hospitals, 1.7 to 5 aggressive attacks per patient-year were reported. If talking to the patient has no calming effect, intervention with drugs is required. In this article, we review the evidence on tranquilizing drugs and discuss clinically relevant ethical and practical questions, e.g., with respect to involuntary medication.
Methods: This review is based on pertinent articles retrieved by a selective search in MEDLINE, supplemented by a reference search.
Results: The evidence for the treatment of psychomotor agitation with antipsychotic drugs and benzodiazepines is relatively good. Randomized, controlled trials and a number of Cochrane reviews are available. These publications, however, contain data only on patients who were able to give informed consent. Their findings are often not applicable to real-life emergencies, e.g., when the patient is intoxicated with alcohol or suffers from a pre-existing disease. Haloperidol has a relatively weak effect on aggression when given alone and can also cause side effects such as early dyskinesia and epileptic seizures. It should, therefore, no longer be used as monotherapy. On the other hand, haloperidol combined with benzodiazepines or promethazine and monotherapy with lorazepam, olanzapine, ziprasidone, or aripiprazole intramuscular are effective options for the treatment of aggressive psychomotor agitation.
Conclusion: All of these drugs, if accepted by the patient, can also have an additional, beneficial placebo effect, with the patient calming down more rapidly than could be explained on pharmacological grounds alone. It is, therefore, important in emergencies (as at other times) for the patient to be involved in treatment decisions to the greatest possible extent.
Figures
Comment in
-
Therapeutic Drug Monitoring.Dtsch Arztebl Int. 2019 Oct 11;116(41):691. doi: 10.3238/arztebl.2019.0691a. Dtsch Arztebl Int. 2019. PMID: 31709976 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2019 Oct 11;116(41):691. doi: 10.3238/arztebl.2019.0691b. Dtsch Arztebl Int. 2019. PMID: 31709977 Free PMC article. No abstract available.
References
-
- Pajonk FG, Schmitt P, Biedler A, et al. Psychiatric emergencies in prehospital emergency medical systems: a prospective comparison of two urban settings. Gen Hosp Psychiatry. 2008;30:360–366. - PubMed
-
- Ketelsen R, Schulz M, Driessen M. Zwangsmaßnahmen im Vergleich an sechs psychiatrischen Abteilungen. Gesundheitswesen. 2011;73:105–111. - PubMed
-
- Ketelsen R, Zechert C, Driessen M, Schulz M. Characteristics of aggression in the psychiatric hospital and predictors of patients at risk. J Psychiatr Ment Health Nurs. 2007;14:92–99. - PubMed
-
- Scaggs TR, Glass DM, Hutchcraft MG, Weir WB. Prehospital ketamine is a safe and effective treatment for excited delirium in a community hospital based EMS system. Prehosp Disaster Med. 2016;31:563–569. - PubMed
-
- Ho JD, Dawes DM, Nelson RS, et al. Acidosis and catecholamine evaluation following simulated law enforcement „use of force“ encounters. Acad Emerg Med. 20101;7:e60–e68. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical