

Integrative and comparative genomic analyses identify clinically relevant pulmonary carcinoid groups and unveil the supra-carcinoids
- PMID: 31431620
- PMCID: PMC6702229
- DOI: 10.1038/s41467-019-11276-9
Integrative and comparative genomic analyses identify clinically relevant pulmonary carcinoid groups and unveil the supra-carcinoids
Abstract
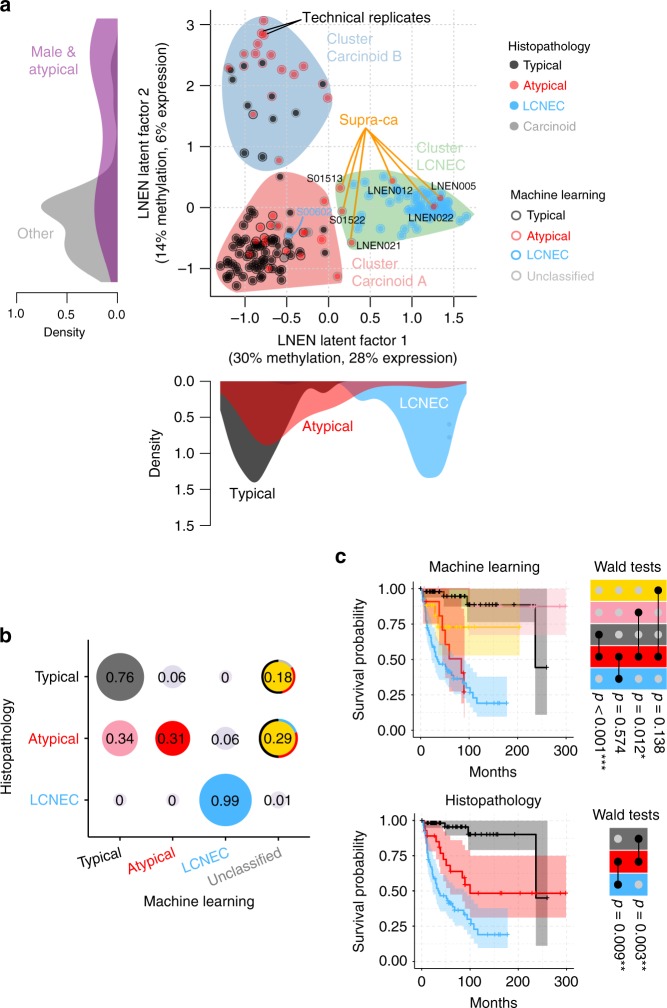
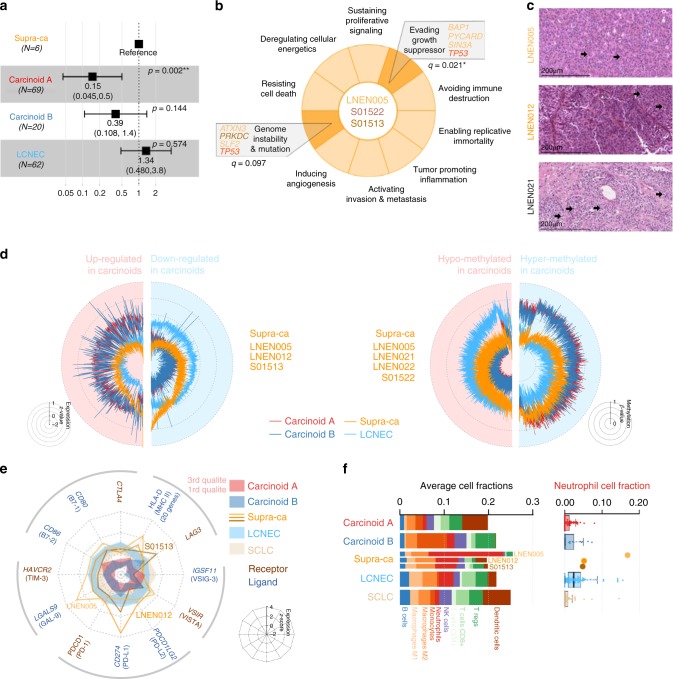
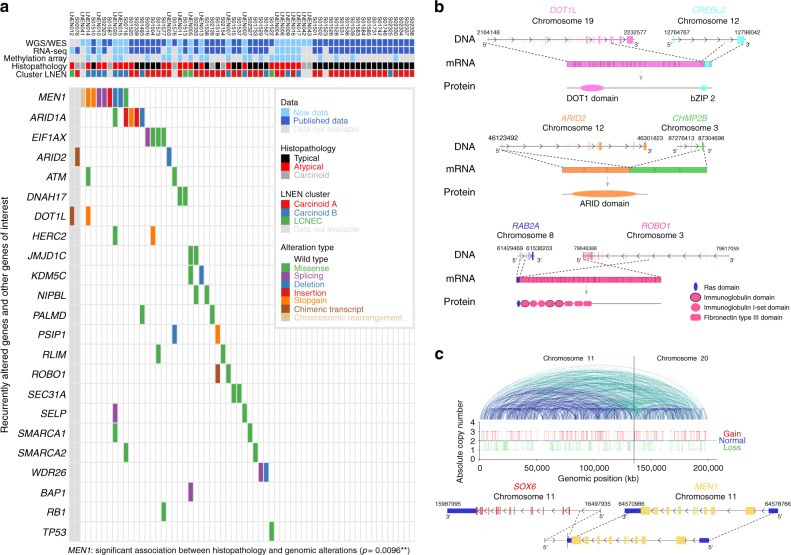
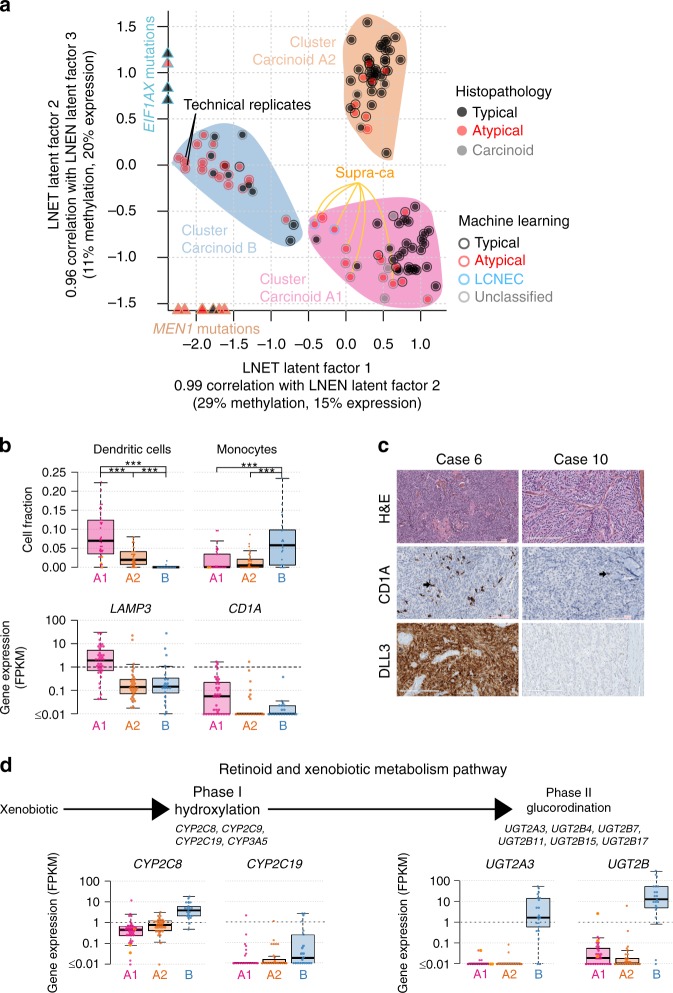
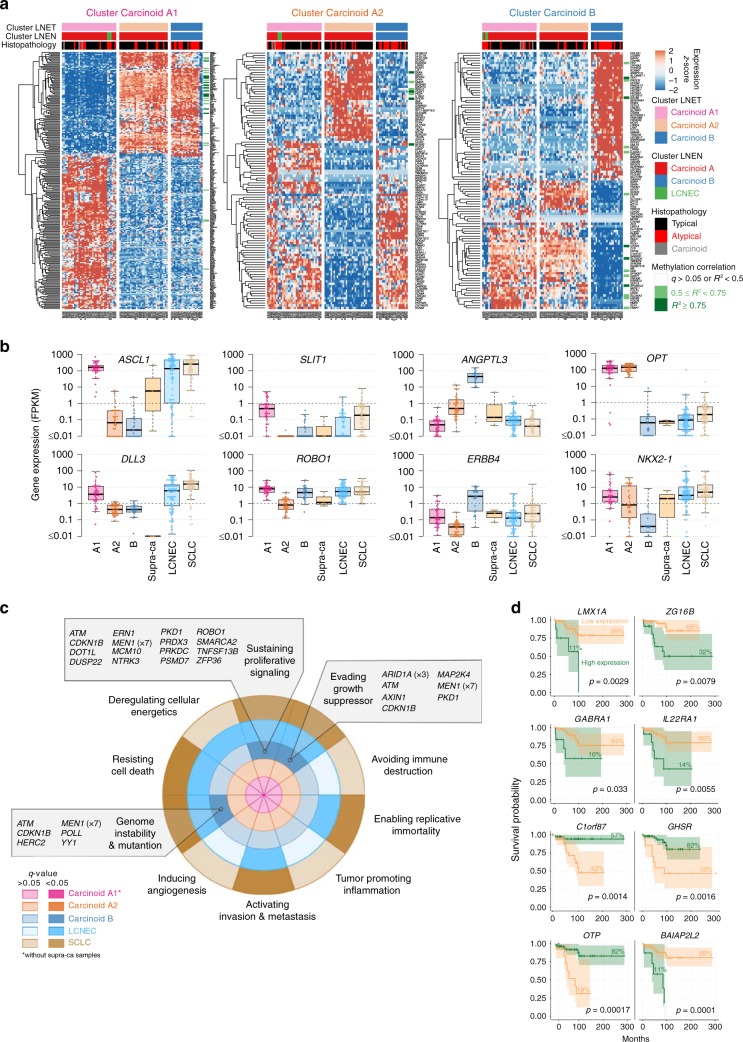
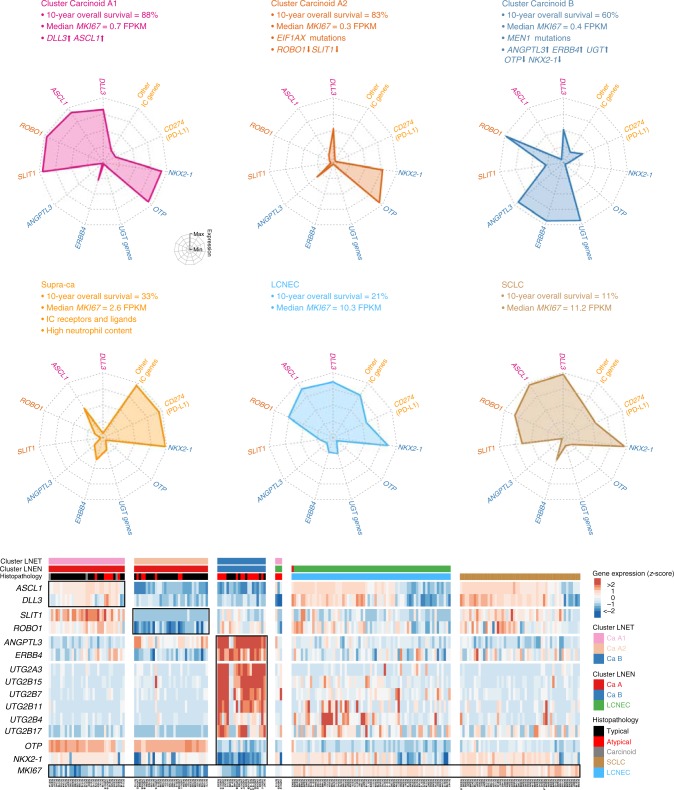
The worldwide incidence of pulmonary carcinoids is increasing, but little is known about their molecular characteristics. Through machine learning and multi-omics factor analysis, we compare and contrast the genomic profiles of 116 pulmonary carcinoids (including 35 atypical), 75 large-cell neuroendocrine carcinomas (LCNEC), and 66 small-cell lung cancers. Here we report that the integrative analyses on 257 lung neuroendocrine neoplasms stratify atypical carcinoids into two prognostic groups with a 10-year overall survival of 88% and 27%, respectively. We identify therapeutically relevant molecular groups of pulmonary carcinoids, suggesting DLL3 and the immune system as candidate therapeutic targets; we confirm the value of OTP expression levels for the prognosis and diagnosis of these diseases, and we unveil the group of supra-carcinoids. This group comprises samples with carcinoid-like morphology yet the molecular and clinical features of the deadly LCNEC, further supporting the previously proposed molecular link between the low- and high-grade lung neuroendocrine neoplasms.
Conflict of interest statement
The authors declare no competing interests. Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organisation, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/World Health Organisation.
Figures
References
-
- Rindi Guido, Klimstra David S., Abedi-Ardekani Behnoush, Asa Sylvia L., Bosman Frederik T., Brambilla Elisabeth, Busam Klaus J., de Krijger Ronald R., Dietel Manfred, El-Naggar Adel K., Fernandez-Cuesta Lynnette, Klöppel Günter, McCluggage W. Glenn, Moch Holger, Ohgaki Hiroko, Rakha Emad A., Reed Nicholas S., Rous Brian A., Sasano Hironobu, Scarpa Aldo, Scoazec Jean-Yves, Travis William D., Tallini Giovanni, Trouillas Jacqueline, van Krieken J. Han, Cree Ian A. A common classification framework for neuroendocrine neoplasms: an International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Modern Pathology. 2018;31(12):1770–1786. doi: 10.1038/s41379-018-0110-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
