

Concussion Guidelines Step 2: Evidence for Subtype Classification
- PMID: 31432081
- PMCID: PMC6911735
- DOI: 10.1093/neuros/nyz332
Concussion Guidelines Step 2: Evidence for Subtype Classification
Abstract
Background: Concussion is a heterogeneous mild traumatic brain injury (mTBI) characterized by a variety of symptoms, clinical presentations, and recovery trajectories. By thematically classifying the most common concussive clinical presentations into concussion subtypes (cognitive, ocular-motor, headache/migraine, vestibular, and anxiety/mood) and associated conditions (cervical strain and sleep disturbance), we derive useful definitions amenable to future targeted treatments.
Objective: To use evidence-based methodology to characterize the 5 concussion subtypes and 2 associated conditions and report their prevalence in acute concussion patients as compared to baseline or controls within 3 d of injury.
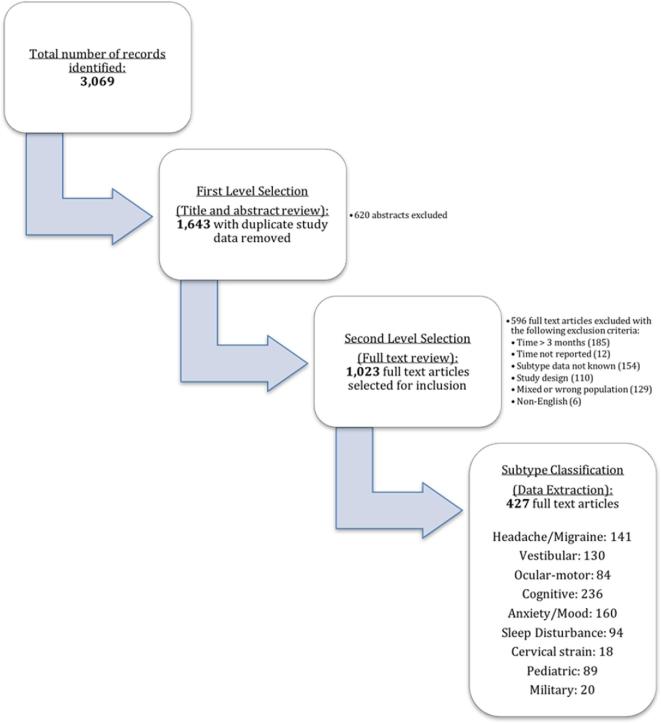
Methods: A multidisciplinary expert workgroup was established to define the most common concussion subtypes and their associated conditions and select clinical questions related to prevalence and recovery. A literature search was conducted from January 1, 1990 to November 1, 2017. Two experts abstracted study characteristics and results independently for each article selected for inclusion. A third expert adjudicated disagreements. Separate meta-analyses were conducted to do the following: 1) examine the prevalence of each subtype/associated condition in concussion patients using a proportion, 2) assess subtype/associated conditions in concussion compared to baseline/uninjured controls using a prevalence ratio, and 3) compare the differences in symptom scores between concussion subtypes and uninjured/baseline controls using a standardized mean difference (SMD).
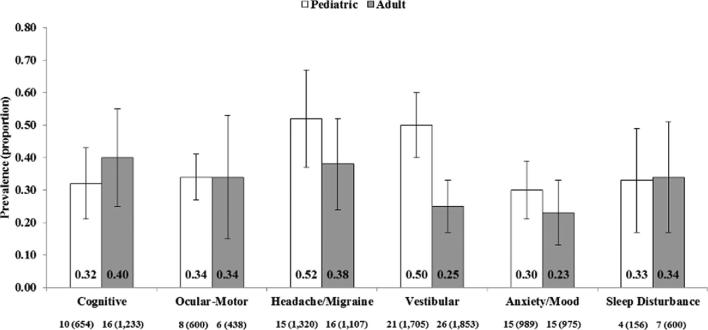
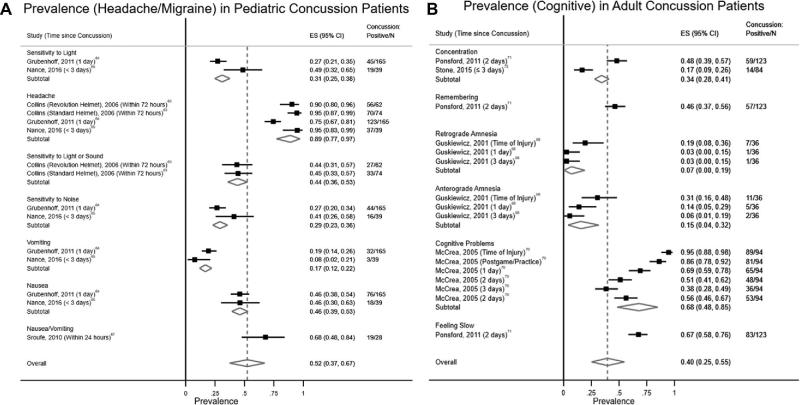
Results: The most prevalent concussion subtypes for pediatric and adult populations were headache/migraine (0.52; 95% CI = 0.37, 0.67) and cognitive (0.40; 95% CI = 0.25, 0.55), respectively. In pediatric patients, the prevalence of the vestibular subtype was also high (0.50; 95% CI = 0.40, 0.60). Adult patients were 4.4, 2.9, and 1.7 times more likely to demonstrate cognitive, vestibular, and anxiety/mood subtypes, respectively, as compared with their controls (P < .05). Children and adults with concussion showed significantly more cognitive symptoms than their respective controls (SMD = 0.66 and 0.24; P < .001). Furthermore, ocular-motor in adult patients (SMD = 0.72; P < .001) and vestibular symptoms in both pediatric and adult patients (SMD = 0.18 and 0.36; P < .05) were significantly worse in concussion patients than in controls.
Conclusion: Five concussion subtypes with varying prevalence within 3 d following injury are commonly seen clinically and identifiable upon systematic literature review. Sleep disturbance, a concussion-associated condition, is also common. There was insufficient information available for analysis of cervical strain. A comprehensive acute concussion assessment defines and characterizes the injury and, therefore, should incorporate evaluations of all 5 subtypes and associated conditions.
Keywords: Concussion; head injury; meta-analysis; mild traumatic brain injury; oculomotor; subtype; systematic review; traumatic brain injury; vestibular.
© Congress of Neurological Surgeons 2019.
Figures
Comment in
-
Commentary: Concussion Guidelines Step 2: Evidence for Subtype Classification.Neurosurgery. 2020 Feb 1;86(2):E222-E223. doi: 10.1093/neuros/nyz364. Neurosurgery. 2020. PMID: 31515561 No abstract available.
-
Commentary: Concussion Guidelines Step 2: Evidence for Subtype Classification.Neurosurgery. 2020 Feb 1;86(2):E224. doi: 10.1093/neuros/nyz365. Neurosurgery. 2020. PMID: 31529054 No abstract available.
-
Commentary: Concussion Guidelines Step 2: Evidence for Subtype Classification.Neurosurgery. 2020 Jan 1;86(1):E1. doi: 10.1093/neuros/nyz426. Neurosurgery. 2020. PMID: 31670378 No abstract available.
References
-
- Carney N, Ghajar J, Jagoda A et al. .. Concussion guidelines step 1. Neurosurgery. 2014;75(suppl 1):S3-S15. - PubMed
-
- McCrory P, Meeuwisse W, Dvorak J et al. .. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2017;51(11):838-847. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
