

Population Pharmacokinetics of Intravenous Salbutamol in Children with Refractory Status Asthmaticus
- PMID: 31432470
- PMCID: PMC7007440
- DOI: 10.1007/s40262-019-00811-y
Population Pharmacokinetics of Intravenous Salbutamol in Children with Refractory Status Asthmaticus
Abstract
Background: Intravenous salbutamol is used to treat children with refractory status asthmaticus, however insufficient pharmacokinetic data are available to guide initial and subsequent dosing recommendations for its intravenous use. The pharmacologic activity of salbutamol resides predominantly in the (R)-enantiomer, with little or no activity and even concerns of adverse reactions attributed to the (S)-enantiomer.
Objective: Our aim was to develop a population pharmacokinetic model to characterize the pharmacokinetic profile for intravenous salbutamol in children with status asthmaticus admitted to the pediatric intensive care unit (PICU), and to use this model to study the effect of different dosing schemes with and without a loading dose.
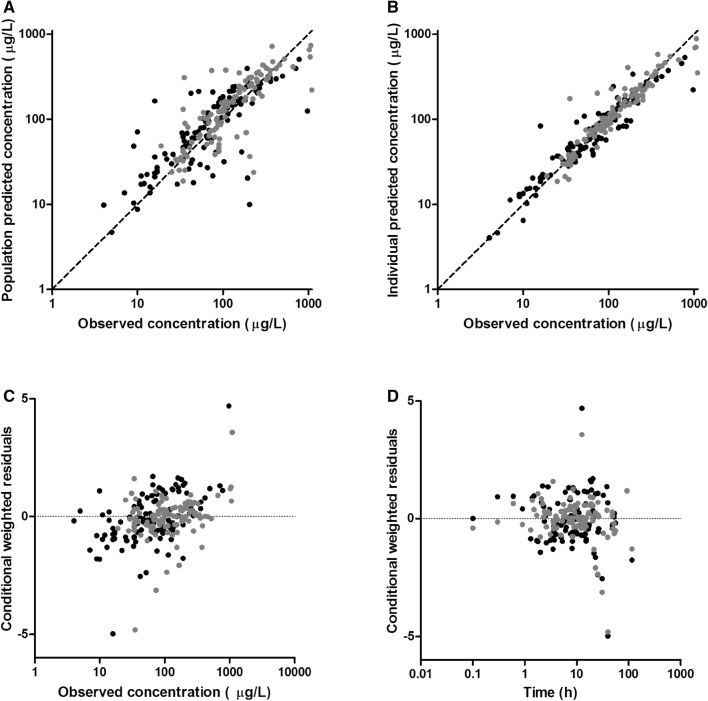
Methods: From 19 children (median age 4.9 years [range 9 months-15.3 years], median weight 18 kg [range 7.8-70 kg]) treated with continuous intravenous salbutamol at the PICU, plasma samples for R- and S-salbutamol concentrations (111 samples), as well as asthma scores, were collected prospectively at the same time points. Possible adverse reactions and patients' clinical data (age, sex, weight, drug doses, liver and kidney function) were recorded. With these data, a population pharmacokinetic model was developed using NONMEM 7.2. After validation, the model was used for simulations to evaluate the effect of different dosing regimens with or without a loading dose.
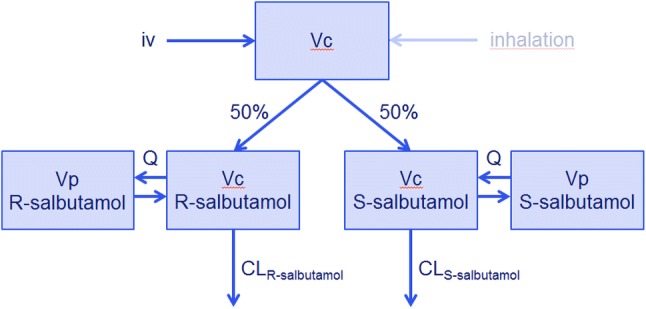
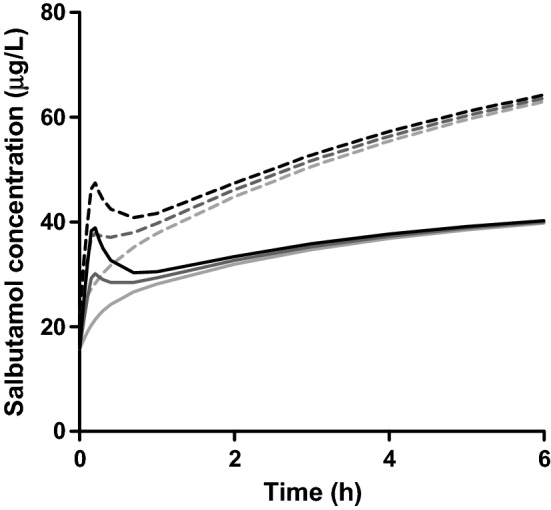
Results: A two-compartment model with separate clearance for R- and S-salbutamol (16.3 L/h and 8.8 L/h, respectively) best described the data. Weight was found to be a significant covariate for clearance and volume of distribution. No other covariates were identified. Simulations showed that a loading dose can result in higher R-salbutamol concentrations in the early phase after the start of infusion therapy, preventing accumulation of S-salbutamol.
Conclusions: The pharmacokinetic model of intravenous R- and S-salbutamol described the data well and showed that a loading dose should be considered in children. This model can be used to evaluate the pharmacokinetic-pharmacodynamic relationship of intravenous salbutamol in children, and, as a next step, the effectiveness and tolerability of intravenous salbutamol in children with severe asthma.
Conflict of interest statement
Nienke J. Vet, Brenda C.M. de Winter, Muriel Koninckx, Shelley A. Boeschoten, Annemie L.M. Boehmer, Jacintha T. Verhallen, Frans B. Plötz, Anja A. Vaessen-Verberne, Bart C.H. van der Nagel, Catherijne A.J. Knibbe, Corinne M.P. Buysse, Saskia N. de Wildt, Birgit C.P. Koch, and Matthijs de Hoog declare they have no potential conflicts of interest that might be relevant to the contents of this manuscript.
Figures
References
-
- Boeschoten SA, Buysse CMP, Merkus P, van Wijngaarden JMC, Heisterkamp SGJ, de Jongste JC, SKIC Dutch Collaborative PICU Research Network et al. Children with severe acute asthma admitted to Dutch PICUs: a changing landscape. Pediatr Pulmonol. 2018;53(7):857–865. doi: 10.1002/ppul.24009. - DOI - PMC - PubMed
-
- British guideline on the management of asthma: a national clinical guideline. 2016. Available at: https://www.brit-thoracic.org.uk/document-library/clinical-information/a....
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
