

Neuropathologic basis of frontotemporal dementia in progressive supranuclear palsy
- PMID: 31433871
- PMCID: PMC6899964
- DOI: 10.1002/mds.27816
Neuropathologic basis of frontotemporal dementia in progressive supranuclear palsy
Abstract
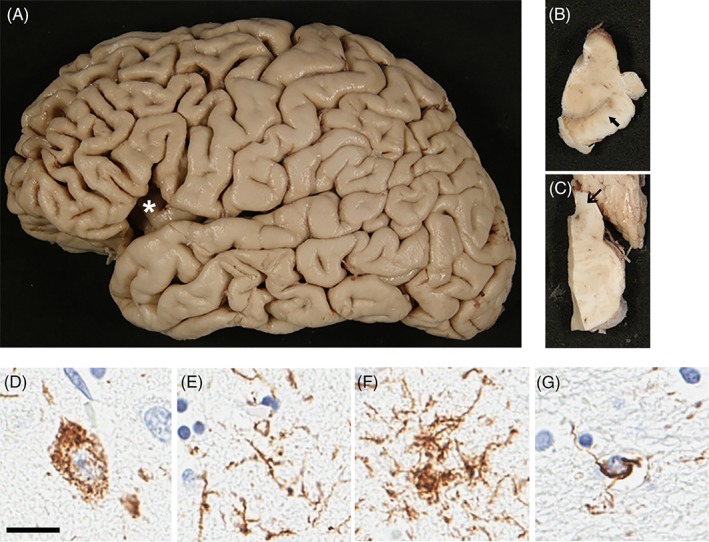
Background: Progressive supranuclear palsy (PSP) is a neurodegenerative disorder characterized by neuronal loss in the extrapyramidal system with pathologic accumulation of tau in neurons and glia. The most common clinical presentation of PSP, referred to as Richardson syndrome, is that of atypical parkinsonism with vertical gaze palsy, axial rigidity, and frequent falls. Although cognitive deficits in PSP are often ascribed to subcortical dysfunction, a subset of patients has dementia with behavioral features similar to the behavioral variant of frontotemporal dementia. In this study we aimed to identify the clinical and pathological characteristics of PSP presenting with frontotemporal dementia.
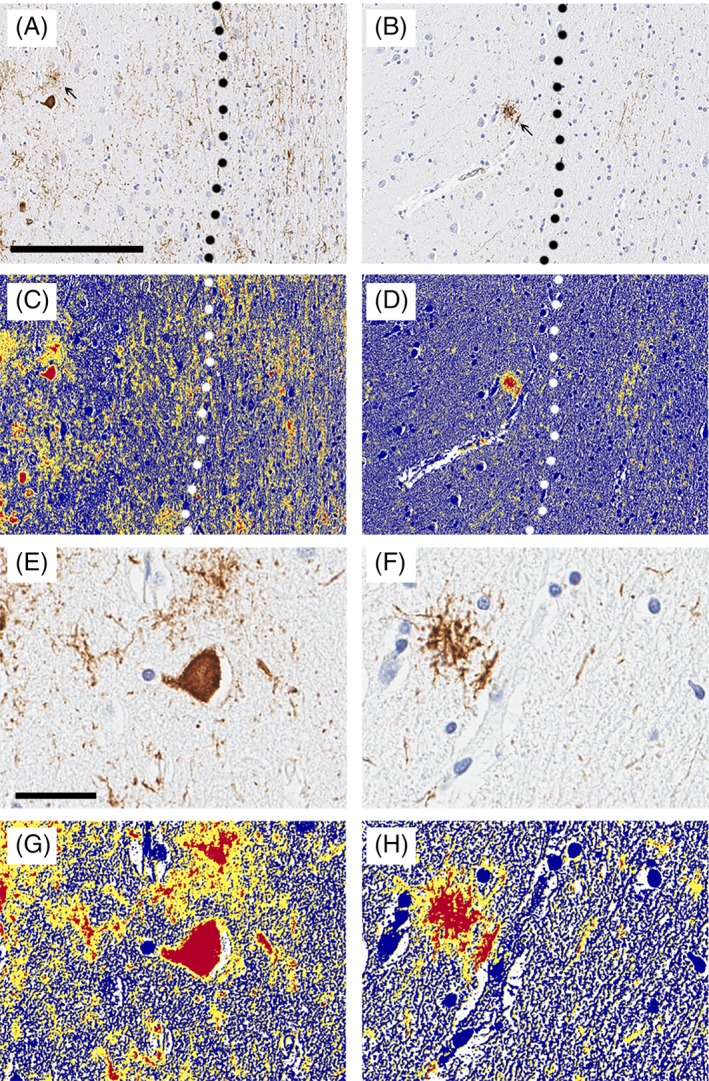
Methods: In this study, we compared clinical and pathologic characteristics of 31 patients with PSP with Richardson syndrome with 15 patients with PSP with frontotemporal dementia. For pathological analysis, we used semiquantitative methods to assess neuronal and glial lesions with tau immunohistochemistry, as well image analysis of tau burden using digital microscopic methods.
Results: We found greater frontal and temporal neocortical neuronal tau pathology in PSP with frontotemporal dementia compared with PSP with Richardson syndrome. White matter tau pathology was also greater in PSP with frontotemporal dementia than PSP with Richardson syndrome. Genetic and demographic factors were not associated with atypical distribution of tau pathology in PSP with frontotemporal dementia.
Conclusions: The results confirm the subset of cognitive-predominant PSP mimicking frontotemporal dementia in PSP. PSP with frontotemporal dementia has distinct clinical features that differ from PSP with Richardson syndrome, as well as differences in distribution and density of tau pathology. © 2019 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Keywords: behavioral variant frontotemporal dementia; immunohistochemistry, image analysis; progressive supranuclear palsy; tau.
© 2019 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Figures
References
-
- Dickson DW, Ahmed Z, Algom AA, Tsuboi Y, Josephs KA. Neuropathology of variants of progressive supranuclear palsy. Curr Opin Neurol 2010;23(4):394–400. - PubMed
-
- Williams DR, de Silva R, Paviour DC, et al. Characteristics of two distinct clinical phenotypes in pathologically proven progressive supranuclear palsy: Richardson's syndrome and PSP‐parkinsonism. Brain 2005;128(Pt 6):1247–1258. - PubMed
-
- Hassan A, Parisi JE, Josephs KA. Autopsy‐proven progressive supranuclear palsy presenting as behavioral variant frontotemporal dementia. Neurocase 2012;18(6):478–488. - PubMed
-
- Respondek G, Stamelou M, Kurz C, et al. The phenotypic spectrum of progressive supranuclear palsy: a retrospective multicenter study of 100 definite cases. Mov Disord 2014;29(14):1758–1766. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
