

Antibody Therapies for Acute Myeloid Leukemia: Unconjugated, Toxin-Conjugated, Radio-Conjugated and Multivalent Formats
- PMID: 31434267
- PMCID: PMC6723634
- DOI: 10.3390/jcm8081261
Antibody Therapies for Acute Myeloid Leukemia: Unconjugated, Toxin-Conjugated, Radio-Conjugated and Multivalent Formats
Abstract
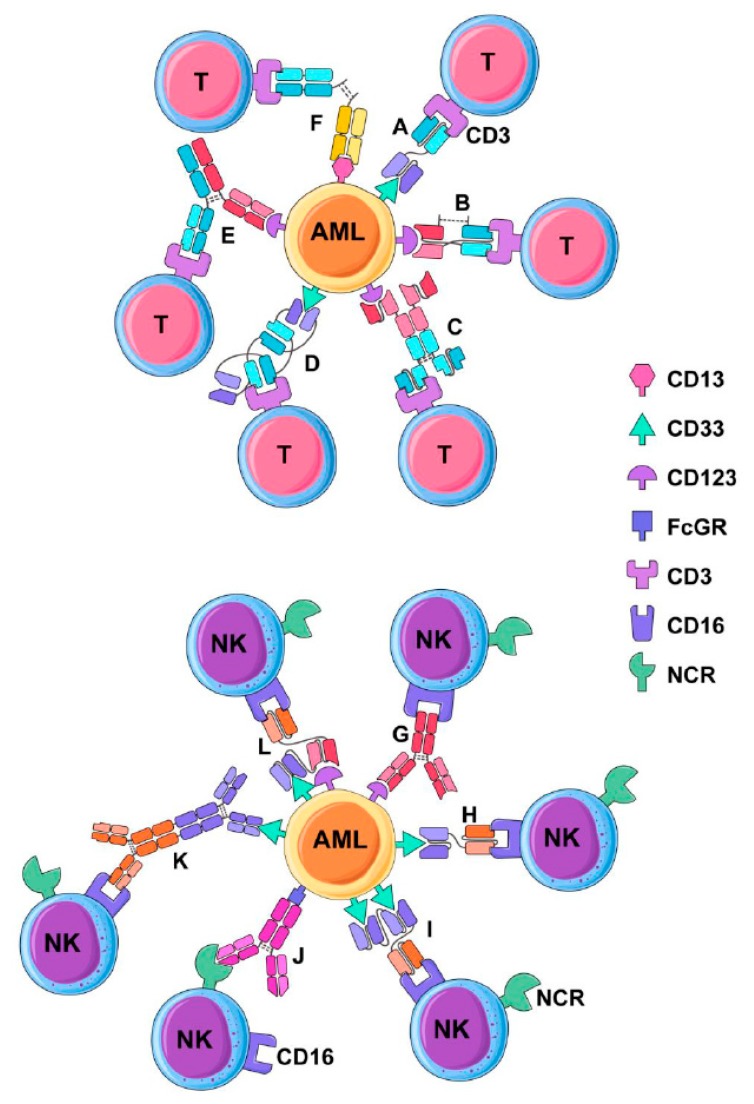
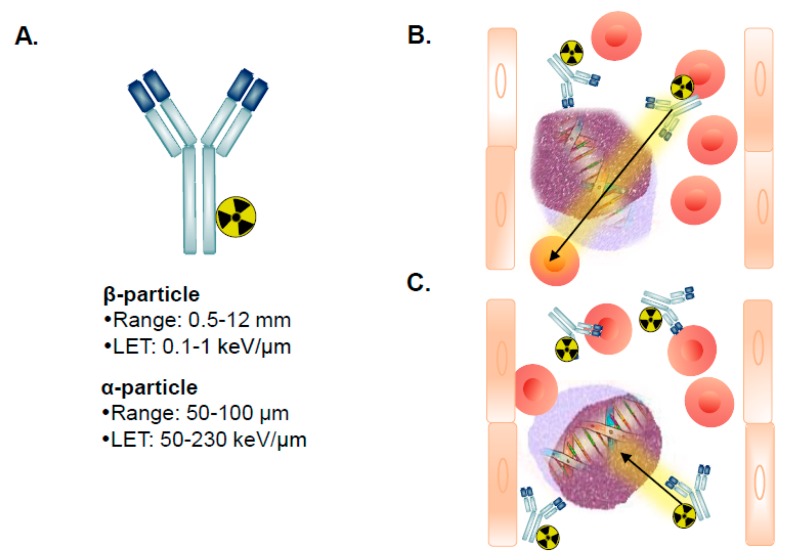
In recent decades, therapy for acute myeloid leukemia (AML) has remained relatively unchanged, with chemotherapy regimens primarily consisting of an induction regimen based on a daunorubicin and cytarabine backbone, followed by consolidation chemotherapy. Patients who are relapsed or refractory can be treated with allogeneic hematopoietic stem-cell transplantation with modest benefits to event-free and overall survival. Other modalities of immunotherapy include antibody therapies, which hold considerable promise and can be categorized into unconjugated classical antibodies, multivalent recombinant antibodies (bi-, tri- and quad-specific), toxin-conjugated antibodies and radio-conjugated antibodies. While unconjugated antibodies can facilitate Natural Killer (NK) cell antibody-dependent cell-mediated cytotoxicity (ADCC), bi- and tri-specific antibodies can engage either NK cells or T-cells to redirect cytotoxicity against AML targets in a highly efficient manner, similarly to classic ADCC. Finally, toxin-conjugated and radio-conjugated antibodies can increase the potency of antibody therapies. Several AML tumour-associated antigens are at the forefront of targeted therapy development, which include CD33, CD123, CD13, CLL-1 and CD38 and which may be present on both AML blasts and leukemic stem cells. This review focused on antibody therapies for AML, including pre-clinical studies of these agents and those that are either entering or have been tested in early phase clinical trials. Antibodies for checkpoint inhibition and microenvironment targeting in AML were excluded from this review.
Keywords: AML; acute myeloid leukemia; antibody; bi-specific antibody; therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- McLaughlin P., Grillo-López A.J., Link B.K., Levy R., Czuczman M.S., Williams M.E., Heyman M.R., Bence-Bruckler I., White C.A., Cabanillas F., et al. Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: Half of patients respond to a four-dose treatment program. J. Clin. Oncol. 1998;16:2825–2833. doi: 10.1200/JCO.1998.16.8.2825. - DOI - PubMed
-
- Yates J.W. Cytosine arabinoside (NSC-63878) and daunorubicin (NSC-83142) therapy in acute nonlymphocytic leukemia. Cancer Chemother. Rep. 1973;57:485–488. - PubMed
-
- Rai K.R., Holland J.F., Glidewell O.J., Weinberg V., Brunner K., Obrecht J.P., Preisler H.D., Nawabi I.W., Prager D., Carey R.W., et al. Treatment of acute myelocytic leukemia: A study by cancer and leukemia group B. Blood. 1981;58:1203–1212. - PubMed
-
- Yates J., Glidewell O., Wiernik P., Cooper M.R., Steinberg D., Dosik H., Levy R., Hoagland C., Henry P., Gottlieb A., et al. Cytosine arabinoside with daunorubicin or adriamycin for therapy of acute myelocytic leukemia: A CALGB study. Blood. 1982;60:454–462. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
