

Cardiac mucormycosis: a case report
- PMID: 31436824
- PMCID: PMC6764552
- DOI: 10.1093/ehjcr/ytz130
Cardiac mucormycosis: a case report
Abstract
Background: Mucormycosis is an invasive fungal infection (IFI) most commonly seen in immunocompromised patients. Diabetic ketoacidosis, haematopoietic transplantation, iron overload states, and deferoxamine therapy are considered to be some of the classical risk factors. While cutaneous and rhino-sinusoidal forms may be seen in immunocompetent (IC) individuals, cardiac and mediastinal involvement is rare. In this report, we describe a young patient without predisposing factors who presented as mediastinal mucormycosis with extensive cardiac involvement.
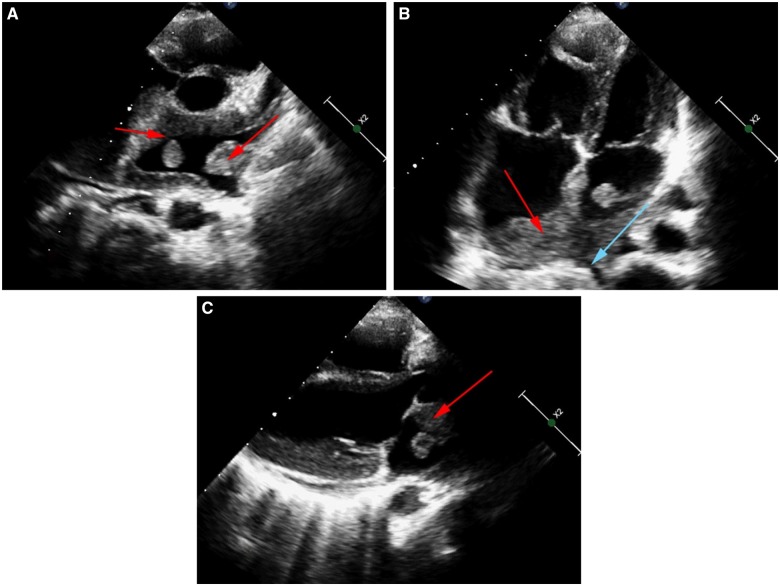
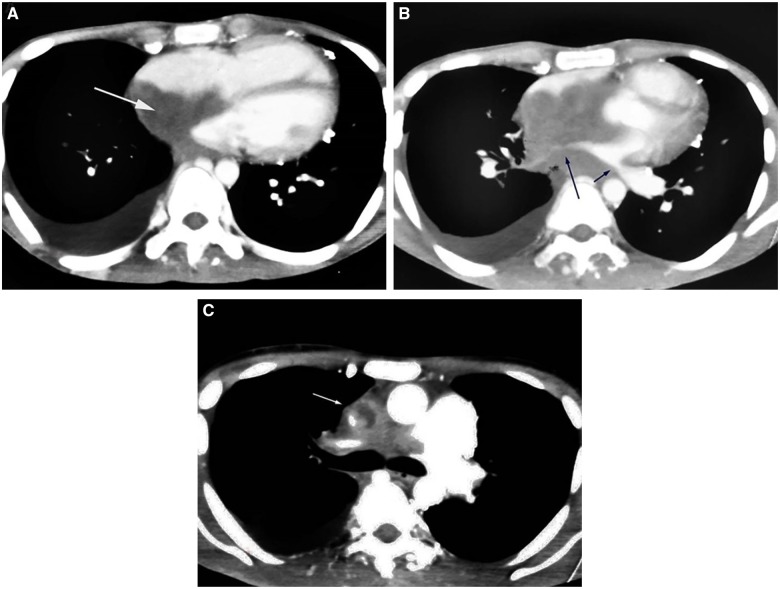
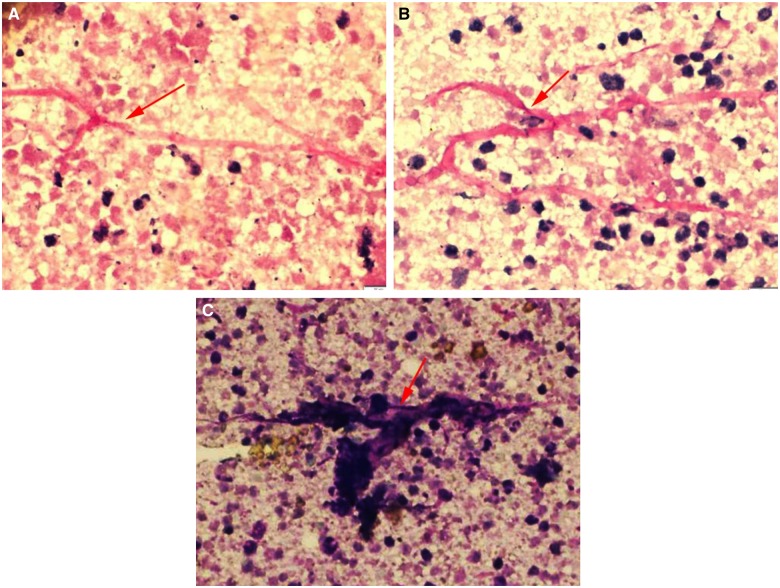
Case summary: A 19-year-old male presented with complaints of dry cough and dyspnoea on exertion over the last 4 months. Echocardiography showed diffuse infiltration of both atria along with multiple pedunculated freely mobile masses. A computed tomography chest was done to further delineate the true extent of the disease and revealed diffuse infiltration of the mediastinum, bilateral atria and interatrial septum, pulmonary veins, and superior vena cava. A fine needle aspiration cytology from a mediastinal mass revealed broad aseptate fungal hyphae with right angled branching consistent with Mucor. Extensive evaluation could not find any predisposing factors. The patient was started on Amphotericin B and surgical debridement was contemplated. However, owing to the diffuse infiltration around the heart and mediastinal vasculature, debridement could not be performed and the patient eventually succumbed to the illness.
Discussion: Mediastinal mucormycosis though rare in IC patients, is a rapidly progressive condition with a high fatality. A high index of suspicion needs to be maintained in individuals presenting with infiltrative disorders of the mediastinum for early diagnosis and prompt treatment.
Keywords: Immunocompromise; Cardiac mucormycosis; Case report; Immunocompetent; Invasive fungal infection; Mediastinal mucormycosis.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

References
-
- Chayakulkeeree M, Ghannoum MA, Perfect JR.. Zygomycosis: the re-emerging fungal infection. Eur J Clin Microbiol Infect Dis 2006;25:215–229. - PubMed
-
- Mignogna MD, Fortuna G, Leuci S, Adamo D, Ruoppo E, Siano M, Mariani U.. Mucormycosis in immunocompetent patients: a case-series of patients with maxillary sinus involvement and a critical review of the literature. Int J Infect Dis 2011;15:e533–e540. - PubMed
-
- Hibbett DS, Binder M, Bischoff JF, Blackwell M, Cannon PF, Eriksson OE, Huhndorf S, James T, Kirk PM, Lücking R, Thorsten Lumbsch H, Lutzoni F, Matheny PB, McLaughlin DJ, Powell MJ, Redhead S, Schoch CL, Spatafora JW, Stalpers JA, Vilgalys R, Aime MC, Aptroot A, Bauer R, Begerow D, Benny GL, Castlebury LA, Crous PW, Dai Y-C, Gams W, Geiser DM, Griffith GW, Gueidan C, Hawksworth DL, Hestmark G, Hosaka K, Humber RA, Hyde KD, Ironside JE, Kõljalg U, Kurtzman CP, Larsson K-H, Lichtwardt R, Longcore J, Miądlikowska J, Miller A, Moncalvo J-M, Mozley-Standridge S, Oberwinkler F, Parmasto E, Reeb V, Rogers JD, Roux C, Ryvarden L, Sampaio JP, Schüßler A, Sugiyama J, Thorn RG, Tibell L, Untereiner WA, Walker C, Wang Z, Weir A, Weiss M, White MM, Winka K, Yao Y-J, Zhang N.. A higher-level phylogenetic classification of the fungi. Mycol Res 2007;111:509–547. - PubMed
-
- Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, Schaufele RL, Sein M, Sein T, Chiou CC, Chu JH, Kontoyiannis DP, Walsh TJ.. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis 2005;41:634–653. - PubMed
-
- Virmani R, Connor DH, McAllister HA.. Cardiac mucormycosis. A report of five patients and review of 14 previously reported cases. Am J Clin Pathol 1982;78:42–47. - PubMed
LinkOut - more resources
Full Text Sources