

Imaging challenges of immunotherapy and targeted therapy in patients with brain metastases: response, progression, and pseudoprogression
- PMID: 31437274
- PMCID: PMC6954406
- DOI: 10.1093/neuonc/noz147
Imaging challenges of immunotherapy and targeted therapy in patients with brain metastases: response, progression, and pseudoprogression
Abstract
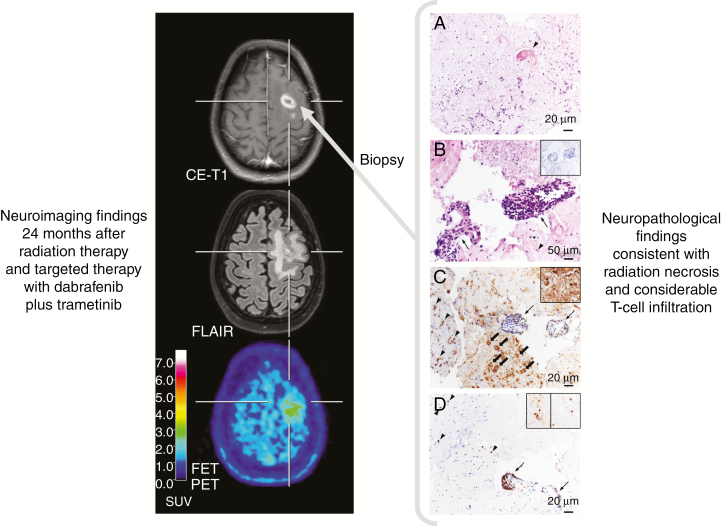
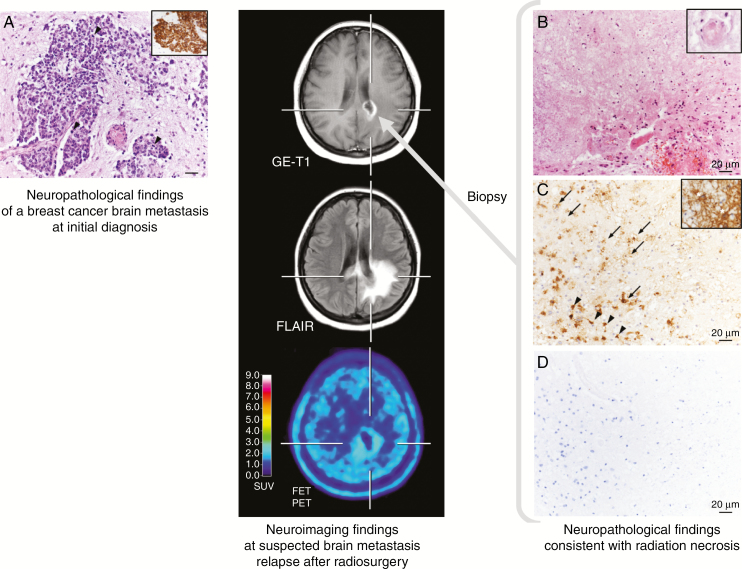
The advent of immunotherapy using immune checkpoint inhibitors (ICIs) and targeted therapy (TT) has dramatically improved the prognosis of various cancer types. However, following ICI therapy or TT-either alone (especially ICI) or in combination with radiotherapy-imaging findings on anatomical contrast-enhanced MRI can be unpredictable and highly variable, and are often difficult to interpret regarding treatment response and outcome. This review aims at summarizing the imaging challenges related to TT and ICI monotherapy as well as combined with radiotherapy in patients with brain metastases, and to give an overview on advanced imaging techniques which potentially overcome some of these imaging challenges. Currently, major evidence suggests that imaging parameters especially derived from amino acid PET, perfusion-/diffusion-weighted MRI, or MR spectroscopy may provide valuable additional information for the differentiation of treatment-induced changes from brain metastases recurrence and the evaluation of treatment response.
Keywords: FET PET; brain metastasis; immune checkpoint inhibitors; lung cancer; melanoma; radiomics.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Long GV, Atkinson V, Lo S, et al. . Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: a multicentre randomised phase 2 study. Lancet Oncol. 2018;19(5):672–681. - PubMed
-
- Stokes WA, Binder DC, Jones BL, et al. . Impact of immunotherapy among patients with melanoma brain metastases managed with radiotherapy. J Neuroimmunol. 2017;313:118–122. - PubMed
