

Trends in EMR for nonmalignant colorectal polyps in the United States
- PMID: 31437455
- PMCID: PMC11044222
- DOI: 10.1016/j.gie.2019.08.004
Trends in EMR for nonmalignant colorectal polyps in the United States
Abstract
Background and aims: Although most large nonpedunculated colorectal lesions can be safely and efficaciously removed using EMR, the use of colectomy for benign colorectal lesions appears to be increasing. The reason(s) is unclear. We aimed to determine the use and adverse events of EMR in the United States.
Methods: We used Optum's de-identified Clinformatics Data Mart Database (2003-2016), a database from a large national insurance provider, to identify all colonoscopies performed with either EMR or simple polypectomy on adult patients from January 1, 2011 to December 31, 2015. We measured time trends, regional variation, and adverse event rates. We assessed risk factors for adverse events using multivariate logistic regression.
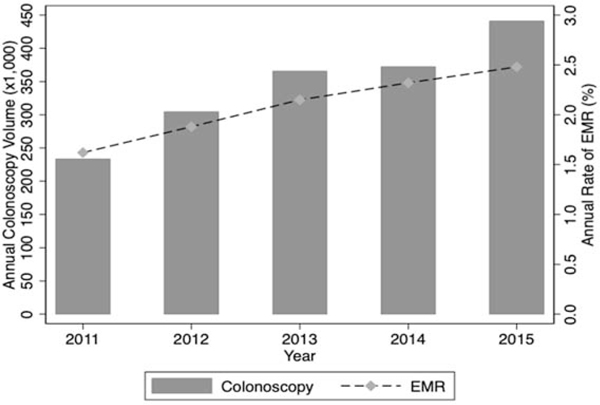
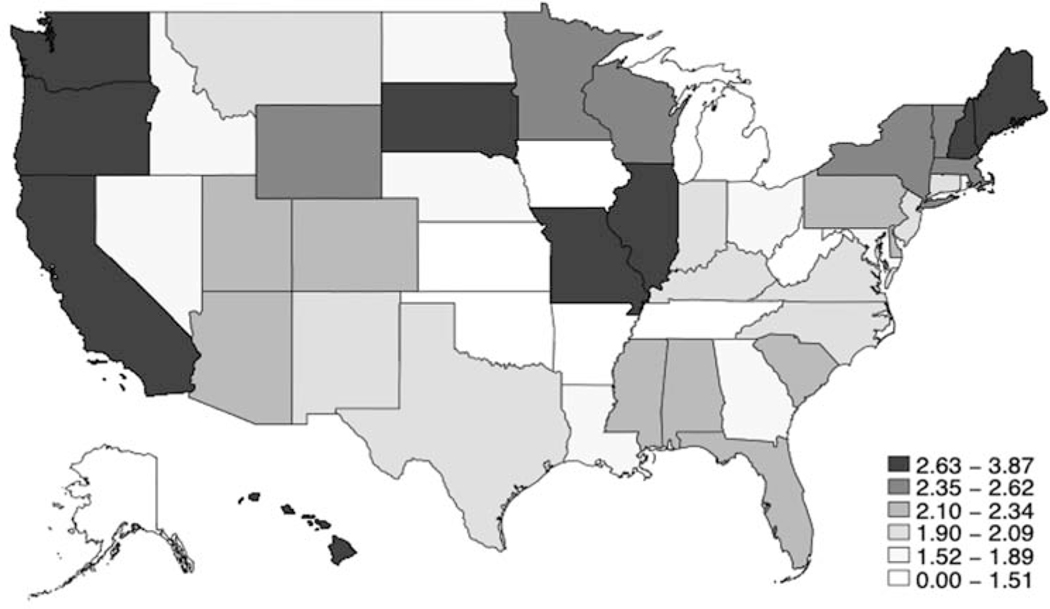
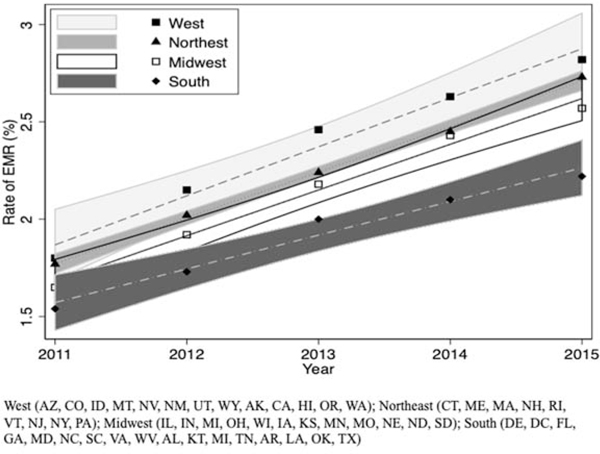
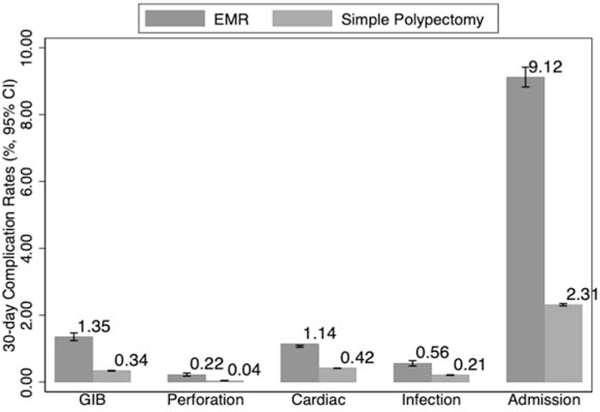
Results: The rate of EMR use in the US increased from 1.62% of all colonoscopies in 2011 to 2.48% of colonoscopies in 2015 (P < .001). There were, however, significant regional differences in the use of EMRs, from 2.4% of colonoscopies in the western United States to 2.0% of colonoscopies in the southern United States. Between 2011 and 2015, we found stable rates of perforation, GI bleeding (GIB), infections, and cardiac adverse events and decreasing rates of admissions after EMR. In our multivariate model, EMR was an independent risk factor for adverse events, albeit the rates of adverse events were low (1.35% GIB, .22% perforation).
Conclusions: Use of EMR is rising in the United States, although there is significant regional variation. The rates of adverse events after EMR and polypectomies were low and stable, confirming the continued safety of EMR procedures. A better understanding of the regional barriers and facilitators may improve the use of EMR as the standard management for benign colorectal lesions throughout the United States.
Copyright © 2020 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
What can colonoscopists do now to move management of large benign laterally spreading lesions in the colorectum from surgery to EMR?Gastrointest Endosc. 2020 Jan;91(1):132-134. doi: 10.1016/j.gie.2019.09.025. Gastrointest Endosc. 2020. PMID: 31865987 No abstract available.
References
-
- Ferlitsch M, Reinhart K, Pramhas S, et al. Sex-specific prevalence of adenomas, advanced adenomas, and colorectal cancer in individuals undergoing screening colonoscopy. JAMA. 2011;306:1352–1358. - PubMed
-
- Keswani RN, Law R, Ciolino JD, et al. Adverse events after surgery for nonmalignant colon polyps are common and associated with increased length of stay and costs. Gastrointest Endosc. 2016;84:296–303 e291. - PubMed
-
- Ahlenstiel G, Hourigan LF, Brown G, et al. Actual endoscopic versus predicted surgical mortality for treatment of advanced mucosal neoplasia of the colon. Gastrointest Endosc. 2014;80:668–676. - PubMed
-
- SwaP, BourkJ, AlexandeS, MosA, Williams SJ. Large refractory colonic polyps: is it time to change our practice? A prospective study of the clinical and economic impact of a tertiary referral colonic mucosal resection and polypectomy service (with videos). Gastrointest Endosc. 2009;70:1128–1136. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
