

A comparison between the Disposcope endoscope and fibreoptic bronchoscope for nasotracheal intubation: a randomized controlled trial
- PMID: 31438861
- PMCID: PMC6706907
- DOI: 10.1186/s12871-019-0834-3
A comparison between the Disposcope endoscope and fibreoptic bronchoscope for nasotracheal intubation: a randomized controlled trial
Abstract
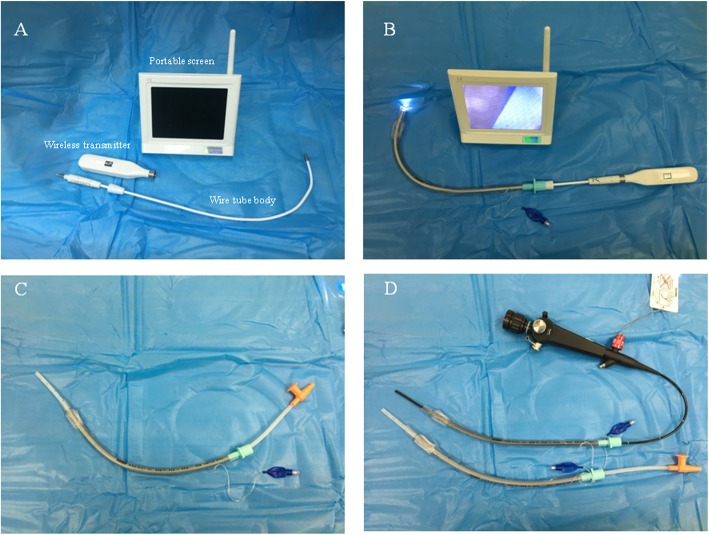
Background: Nasotracheal intubation (NTI) is frequently performed for oral and maxillofacial surgeries. This study evaluated whether NTI is easier when guided by Disposcope endoscopy or fibreoptic bronchoscopy.
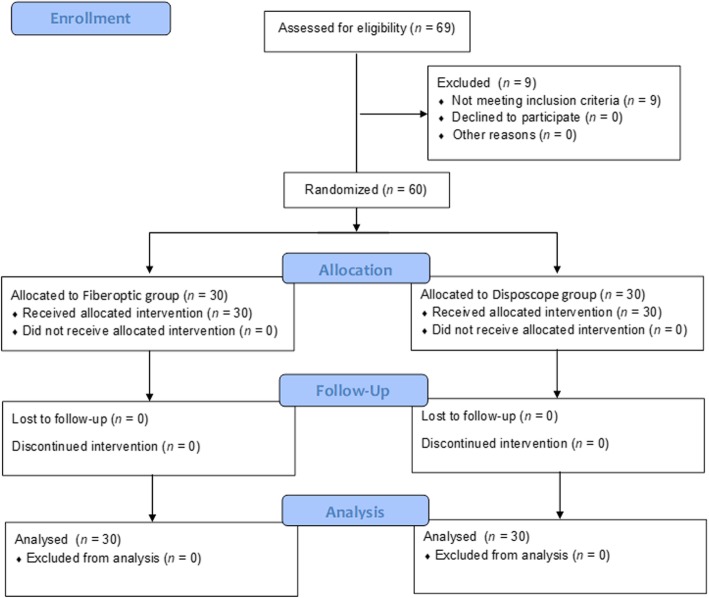
Methods: Sixty patients (30 per group) requiring NTI were randomly assigned to undergo fibreoptic bronchoscopy-guided (fibreoptic group) or Disposcope endoscope-guided (Disposcope group) NTI. The NTI time, which was defined as the time from when the fibreoptic bronchoscope or aseptic suction catheter was inserted into the nasal cavity to the time at which the tracheal tube was correctly inserted through the glottis, was recorded. Epistaxis was evaluated by direct laryngoscopy five minutes after completing NTI and was scored as one of four grades according to the following modified criteria: no epistaxis, mild epistaxis, moderate epistaxis, and severe epistaxis.
Results: The time to complete NTI was significantly longer in the fibreoptic group than in the Disposcope group (38.4 s vs 24.1 s; mean difference, 14.2 s; 95% confidence interval (CI), 10.4 to 18.1). Mild epistaxis was observed in 8 patients in the fibreoptic group and in 7 patients in the Disposcope group (26.7% vs 23.3%, respectively; relative risk, 1.2; 95% CI, 0.4 to 3.9), though no moderate or severe epistaxis occurred in either group. Furthermore, no obvious nasal pain was reported by any of the patients at any time point after extubation (P = 0.74).
Conclusion: NTI can be completed successfully using either fibreoptic bronchoscopy or Disposcope endoscope as a guide without any severe complications. However, compared to fibreoptic bronchoscopy, Disposcope endoscope requires less execution time (the NTI time).
Trial registration: This clinical research was registered at the Chinese Clinical Trial Registry ( www.chictr.org.cn , ChiCTR-IPR-17011462, date of registration, May 2017).
Keywords: Disposcope endoscope; Endotracheal tube; Fibreoptic; Nasotracheal intubation; Video stylet.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Comparison of a tube core and Magill forceps for nasotracheal intubation: a randomised controlled trial.Trials. 2021 Oct 13;22(1):697. doi: 10.1186/s13063-021-05677-9. Trials. 2021. PMID: 34645510 Free PMC article. Clinical Trial.
-
A randomised trial comparing real-time double-lumen endobronchial tube placement with the Disposcope® with conventional blind placement.Anaesthesia. 2017 Sep;72(9):1097-1106. doi: 10.1111/anae.13984. Anaesthesia. 2017. PMID: 28804889 Clinical Trial.
-
A Randomized Trial Comparing the Effect of Fiberoptic Selection and Guidance Versus Random Selection, Blind Insertion, and Direct Laryngoscopy, on the Incidence and Severity of Epistaxis After Nasotracheal Intubation.Anesth Analg. 2018 Aug;127(2):485-489. doi: 10.1213/ANE.0000000000003396. Anesth Analg. 2018. PMID: 29683824 Clinical Trial.
-
Nasotracheal intubation in pediatrics: a narrative review.J Dent Anesth Pain Med. 2024 Apr;24(2):81-90. doi: 10.17245/jdapm.2024.24.2.81. Epub 2024 Mar 28. J Dent Anesth Pain Med. 2024. PMID: 38584754 Free PMC article. Review.
-
Videolaryngoscopy versus direct laryngoscopy for nasotracheal intubation: A systematic review and meta-analysis of randomised controlled trials.J Clin Anesth. 2019 Feb;52:6-16. doi: 10.1016/j.jclinane.2018.08.029. Epub 2018 Aug 25. J Clin Anesth. 2019. PMID: 30153543
Cited by
-
A randomized controlled trail comparing the visual stylet and visual laryngoscope for transoral single lumen tracheal intubation.Sci Rep. 2025 Mar 28;15(1):10733. doi: 10.1038/s41598-025-95298-y. Sci Rep. 2025. PMID: 40155626 Free PMC article. Clinical Trial.
-
Use of the Disposcope endoscope for awake orotracheal intubation in an elderly patient with a large vocal cord polyp -a case report.Korean J Anesthesiol. 2024 Jun;77(3):392-396. doi: 10.4097/kja.23810. Epub 2024 Mar 11. Korean J Anesthesiol. 2024. PMID: 38462978 Free PMC article.
-
Comparison of a tube core and Magill forceps for nasotracheal intubation: a randomised controlled trial.Trials. 2021 Oct 13;22(1):697. doi: 10.1186/s13063-021-05677-9. Trials. 2021. PMID: 34645510 Free PMC article. Clinical Trial.
-
Comparison of video laryngoscope, video stylet, and flexible videoscope for transoral endotracheal intubation in patients with difficult airways: a randomized, parallel-group study.Trials. 2023 Sep 21;24(1):599. doi: 10.1186/s13063-023-07641-1. Trials. 2023. PMID: 37735666 Free PMC article. Clinical Trial.
-
Disposcope endoscope guidance versus fiberoptic bronchoscopy guidance for double-lumen tube intubation in patients undergoing thoracic surgery: a randomized controlled non-inferiority trial.Sci Rep. 2025 Feb 14;15(1):5476. doi: 10.1038/s41598-025-89945-7. Sci Rep. 2025. PMID: 39953079 Free PMC article. Clinical Trial.
References
-
- Sato Boku A, Sobue K, Kako E, Tachi N, Okumura Y, Kanazawa M, Hashimoto M, Harada J. The usefulness of the McGrath MAC laryngoscope in comparison with Airwayscope and Macintosh laryngoscope during routine nasotracheal intubation: a randomaized controlled trial. BMC Anesthesiol. 2017;17(1):160. doi: 10.1186/s12871-017-0451-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
