

Comparison of photoselective green light laser vaporisation versus traditional transurethral resection for benign prostate hyperplasia: an updated systematic review and meta-analysis of randomised controlled trials and prospective studies
- PMID: 31439603
- PMCID: PMC6707662
- DOI: 10.1136/bmjopen-2018-028855
Comparison of photoselective green light laser vaporisation versus traditional transurethral resection for benign prostate hyperplasia: an updated systematic review and meta-analysis of randomised controlled trials and prospective studies
Abstract
Objective: To assess the efficacy and safety of green-light laser photoselective vaporisation of the prostate (PVP) compared with transurethral resection of the prostate (TURP) for lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH).
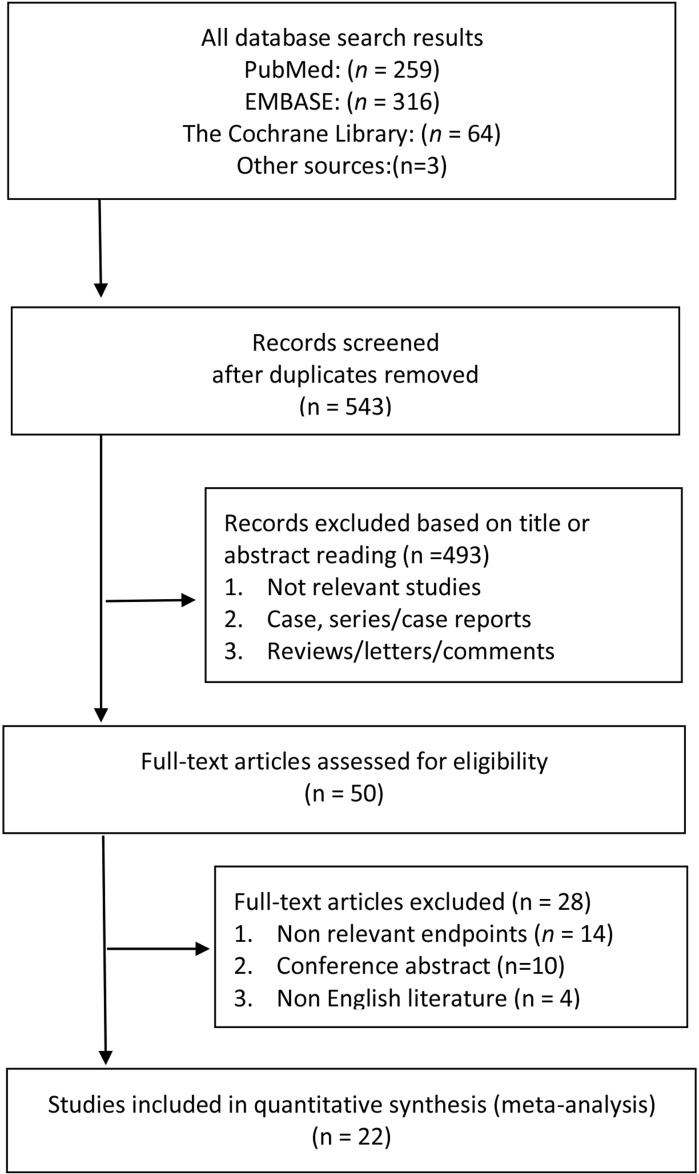
Design: Systematic review and meta-analysis, conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement.
Data sources: PubMed, EMBASE, the Cochrane Library until October 2018.
Eligibility criteria: Randomised controlled trials and prospective studies comparing the safety and efficacy of PVP versus TURP for LUTS manifesting through BPH.
Data extraction and synthesis: Perioperative parameters, complications rates and functional outcomes including treatment-related adverse events such as International Prostate Symptom Score (IPSS), maximum flow rate (Qmax), postvoid residual (PVR), quality of life (QoL) and International Index of Erectile Function (IIEF).
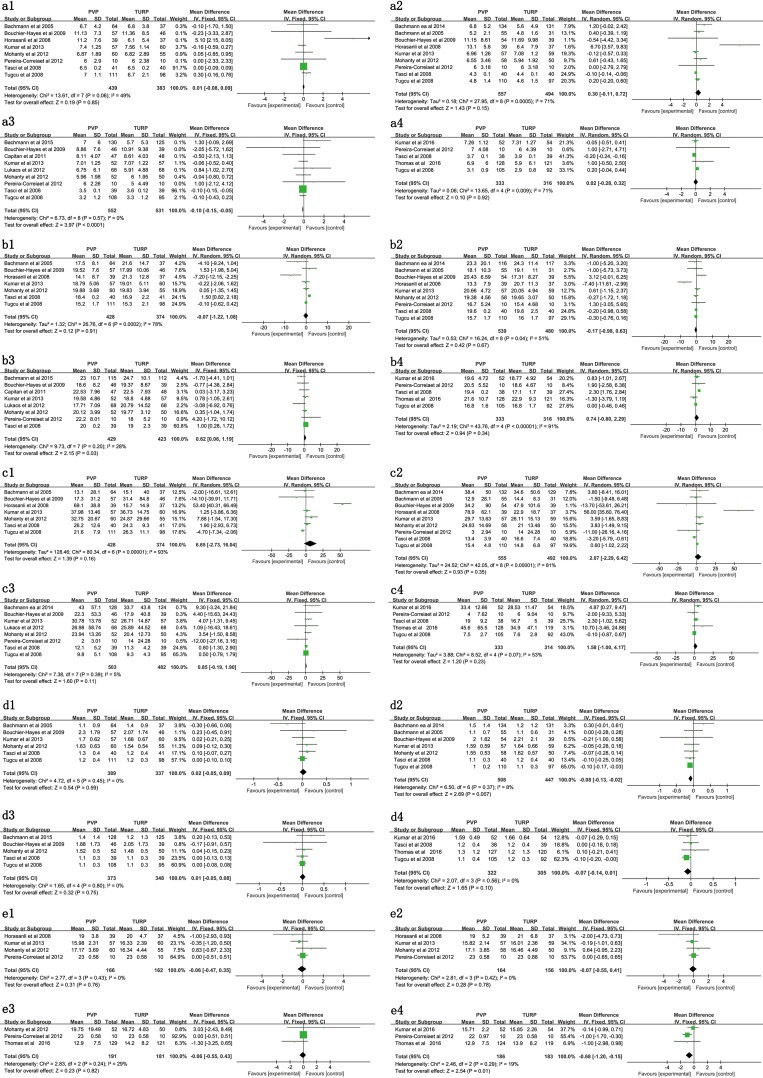
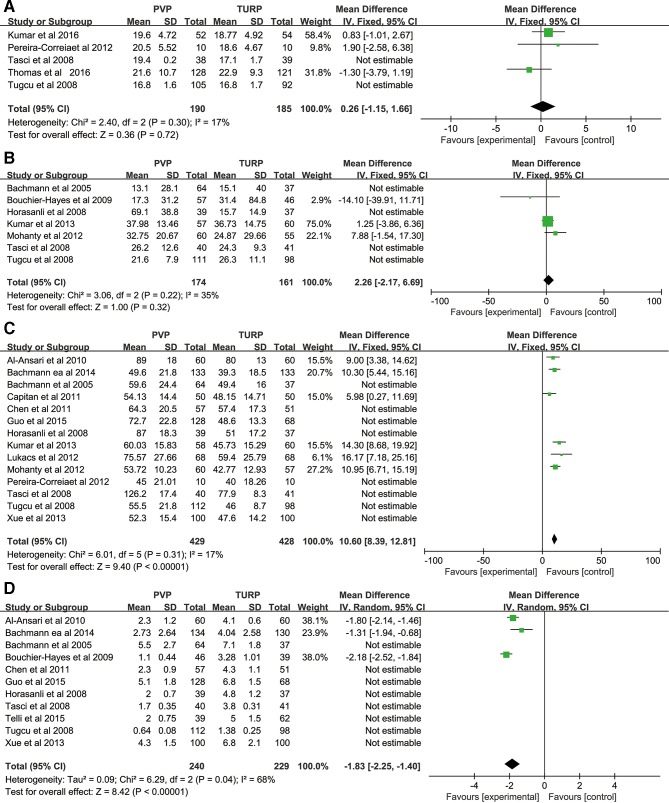
Results: 22 publications consisting of 2665 patients were analysed. Pooled analysis revealed PVP is associated with reduced blood loss, transfusion, clot retention, TUR syndrome, capsular perforation, catheterisation time and hospitalisation, but also with a higher reintervention rate and longer intervention duration (all p<0.05). No significant difference in IPSS, Qmax, QoL, PVR or IIEF at 3, 24, 36 or 60 months was identified. There was a significant difference in QoL at 6 months (MD=-0.08; 95% CI -0.13 to -0.02; p=0.007), and IPSS (MD = -0.10; 95% CI -0.15 to -0.05; p<0.0001) and Qmax (MD=0.62; 95% CI 0.06 to 1.19; p=0.03) at 12 months, although these differences were not clinically relevant.
Conclusion: PVP is an effective alternative, holding additional safety benefits. PVP has equivalent long-term IPSS, Qmax, QoL, PVR, IIEF efficacy and fewer complications. The main drawbacks are dysuria and reintervention, although both can be managed with non-invasive techniques. The additional shortcoming is that PVP does not acquire histological tissue examination which removes an opportunity to identify prostate cancer.
Keywords: benign prostatic hyperplasia (BPH); lower urinary tract symptoms (LUTS); meta-analysis; photoselective vaporisation of the prostate (PVP); transurethral resection of the prostate (TURP).
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Benign Prostatic Hyperplasia.J Urol. 2021 May;205(5):1490-1492. doi: 10.1097/JU.0000000000001665. Epub 2021 Feb 24. J Urol. 2021. PMID: 33625910 No abstract available.
References
-
- Bachmann A, Descazeaud A, Drake M, et al. . Guidelines on the management of non-neurogenic male lower urinary tract symptoms (LUTS), INCL. benign prostatic obstruction (BHO. Madrid, Spain: Presented at 30th Annual EAU Congress, 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials