

Automatic Planning of Whole Breast Radiation Therapy Using Machine Learning Models
- PMID: 31440474
- PMCID: PMC6693433
- DOI: 10.3389/fonc.2019.00750
Automatic Planning of Whole Breast Radiation Therapy Using Machine Learning Models
Abstract
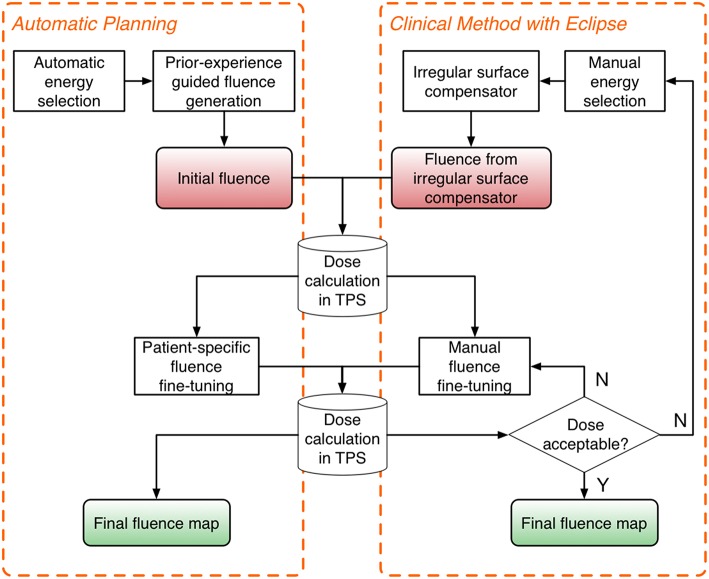
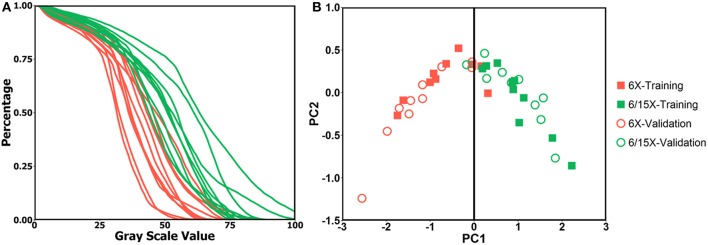
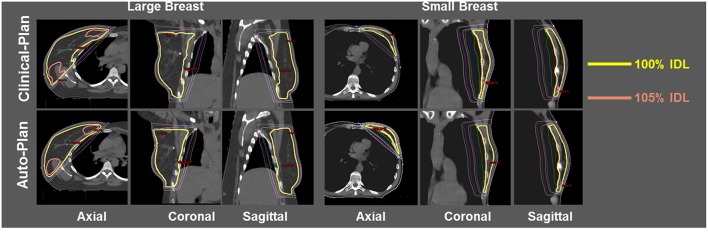
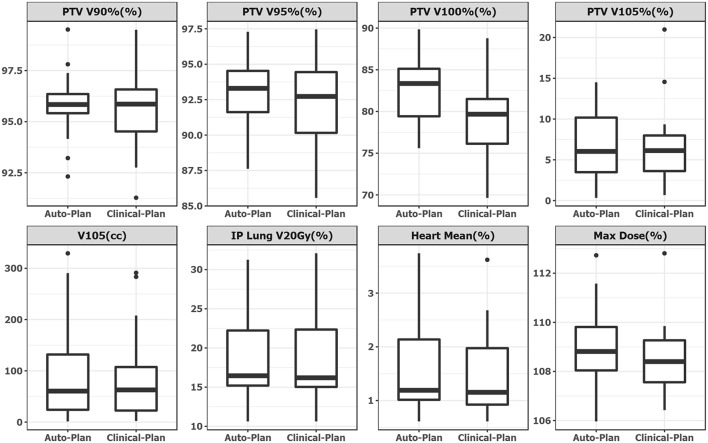
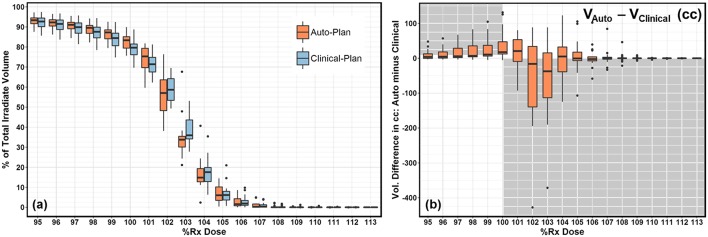
Purpose: To develop an automatic treatment planning system for whole breast radiation therapy (WBRT) based on two intensity-modulated tangential fields, enabling near-real-time planning. Methods and Materials: A total of 40 WBRT plans from a single institution were included in this study under IRB approval. Twenty WBRT plans, 10 with single energy (SE, 6MV) and 10 with mixed energy (ME, 6/15MV), were randomly selected as training dataset to develop the methodology for automatic planning. The rest 10 SE cases and 10 ME cases served as validation. The auto-planning process consists of three steps. First, an energy prediction model was developed to automate energy selection. This model establishes an anatomy-energy relationship based on principle component analysis (PCA) of the gray level histograms from training cases' digitally reconstructed radiographs (DRRs). Second, a random forest (RF) model generates an initial fluence map using the selected energies. Third, the balance of overall dose contribution throughout the breast tissue is realized by automatically selecting anchor points and applying centrality correction. The proposed method was tested on the validation dataset. Non-parametric equivalence test was performed for plan quality metrics using one-sided Wilcoxon Signed-Rank test. Results: For validation, the auto-planning system suggested same energy choices as clinical-plans in 19 out of 20 cases. The mean (standard deviation, SD) of percent target volume covered by 100% prescription dose was 82.5% (4.2%) for auto-plans, and 79.3% (4.8%) for clinical-plans (p > 0.999). Mean (SD) volume receiving 105% Rx were 95.2 cc (90.7 cc) for auto-plans and 83.9 cc (87.2 cc) for clinical-plans (p = 0.108). Optimization time for auto-plan was <20 s while clinical manual planning takes between 30 min and 4 h. Conclusions: We developed an automatic treatment planning system that generates WBRT plans with optimal energy selection, clinically comparable plan quality, and significant reduction in planning time, allowing for near-real-time planning.
Keywords: auto planning; breast cancer; electronic compensation; machine learning; random forest; whole breast radiation therapy.
Figures
References
-
- American Cancer Society. Cancer Facts and Figures 2018. Atlanta: American Cancer Society; (2018).
-
- Jin G-H, Chen L-X, Deng X-W, Liu X-W, Huang Y, Huang X-B. A comparative dosimetric study for treating left-sided breast cancer for small breast size using five different radiotherapy techniques: conventional tangential field, filed-in-filed, Tangential-IMRT, Multi-beam IMRT and VMAT. Radiat Oncol. (2013) 8:89. 10.1186/1748-717X-8-89 - DOI - PMC - PubMed
-
- Yoo S, Blitzblau R, Yin F, Horton JK. Comparison of preoperative partial breast radiosurgery treatment techniques: 3D-CRT, non-coplanar IMRT, coplanar IMRT, and VMAT. Int J Radiat Oncol Biol Phys. (2013) 87:S215 10.1016/j.ijrobp.2013.06.557 - DOI
-
- Vasudevan A, Kariyarambath S, Bhasi S, George PS, Mathew BS. Comparative dosimetric study of 3DCRT, IMRT and VMAT for whole-breast irradiation following breast conservation: a single-institution experience. Int J Radiat Oncol Biol Phys. (2015) 93:E13–E14. 10.1016/j.ijrobp.2015.07.578 - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources