

Implantable cardioverter-defibrillator in Brugada syndrome: Long-term follow-up
- PMID: 31441080
- PMCID: PMC6788474
- DOI: 10.1002/clc.23247
Implantable cardioverter-defibrillator in Brugada syndrome: Long-term follow-up
Abstract
Background: Brugada syndrome (BrS) is associated with sudden cardiac death (SCD). Although implantable cardioverter-defibrillator (ICD) implantation is recommended, the long-term outcomes and follow-up data with regard to ICD complications have led to controversy.
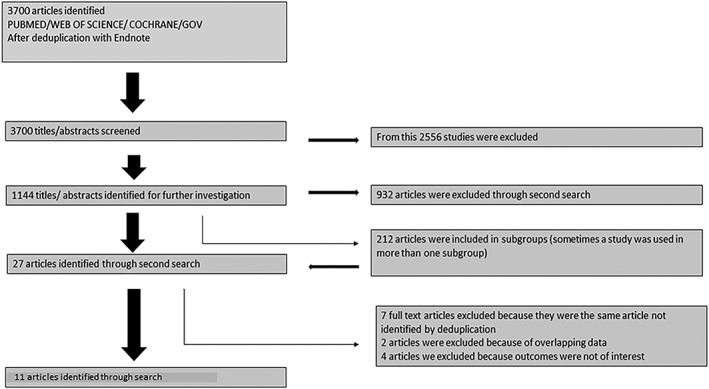
Hypothesis: In the present study, we described the data assimilated in a total of 11 studies, analyzing the outcome in 747 BrS patients receiving ICD.
Methods: Data were performed and analyzed after a systematic review of literature compiled from a thorough database search (PubMed, Web of Science, Cochrane Library, and Cinahl).
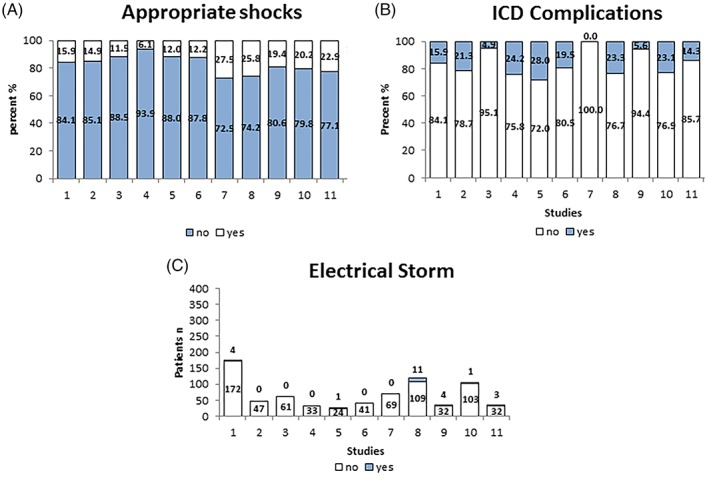
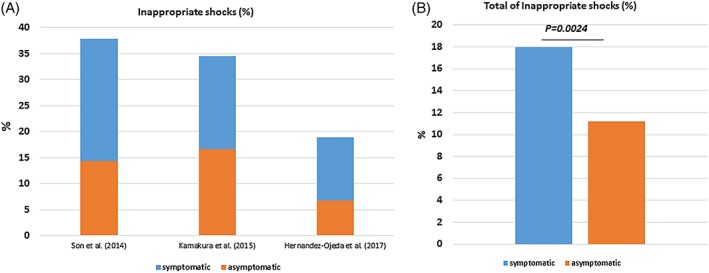
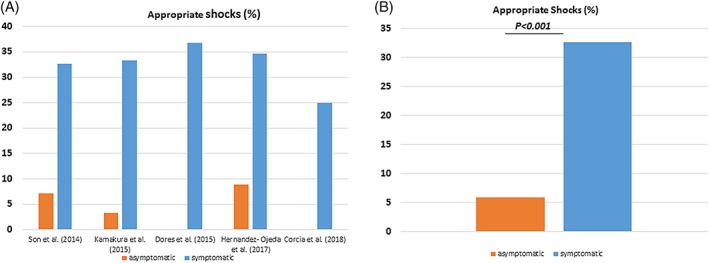
Results: The mean age of patients receiving ICD was (43.1 ± 13.4, 82.5% males, 46.6% spontaneous BrS type I). Around 15.3% of the patients were admitted due to SCD and 10.4% suffered from atrial arrhythmia. Appropriate shocks were documented in 18.1% of the patients over a mean follow-up period of 82.3 months (47.5-110.4). The following complications were recorded: lead failure and fracture (5.4%), lead perforation (0.7%), lead dislodgement (1.7%), infection (3.9%), pain (0.4%), subclavian vein thrombosis (0.3%), pericardial effusion (0.1%), endocarditis (0.1%), psychiatric problems (1.5%), pneumothorax (0.7%). Inappropriate shocks were documented in 18.1% of the patients. The management of inappropriate shocks was achieved by pulmonary vein isolation (0.5%), drug treatment with sotalol (1.3%) or sotalol with beta-blocker (0.3%) and hydroquinidine (0.1%).
Conclusions: ICD therapy in BrS is associated with relevant ICD-related complications including a substantial risk of inappropriate shocks more frequently in symptomatic BrS patients.
Keywords: Brugada; complications; devices; outcome.
© 2019 The Authors. Clinical Cardiology published by Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflict of interests.
Figures
References
-
- Amin AS, Verkerk AO, Bhuiyan ZA, Wilde AA, Tan HL. Novel Brugada syndrome‐causing mutation in ion‐conducting pore of cardiac Na+ channel does not affect ion selectivity properties. Acta Physiol Scand. 2005;185(4):291‐301. - PubMed
-
- Morita H, Nagase S, Kusano K, Ohe T. Spontaneous T wave alternans and premature ventricular contractions during febrile illness in a patient with Brugada syndrome. J Cardiovasc Electrophysiol. 2002;13(8):816‐818. - PubMed
-
- Casado‐Arroyo R, Berne P, Rao JY, Rodriguez‐Manero M, Levinstein M, et al. Long‐term trends in newly diagnosed Brugada syndrome: implications for risk stratification. J Am Coll Cardiol. 2016;68(6):614‐623. - PubMed
-
- Brugada J, Brugada R, Brugada P. Determinants of sudden cardiac death in individuals with the electrocardiographic pattern of Brugada syndrome and no previous cardiac arrest. Circulation. 2003;108(25):3092‐3096. - PubMed
-
- Pappone C, Brugada J, Vicedomini G, et al. Electrical substrate elimination in 135 consecutive patients with Brugada syndrome. Circ Arrhythm Electrophysiol. 2017;10(5):e005053. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
