

Early Experience With Transcatheter Mitral Valve Replacement: A Systematic Review
- PMID: 31441371
- PMCID: PMC6755858
- DOI: 10.1161/JAHA.119.013332
Early Experience With Transcatheter Mitral Valve Replacement: A Systematic Review
Abstract
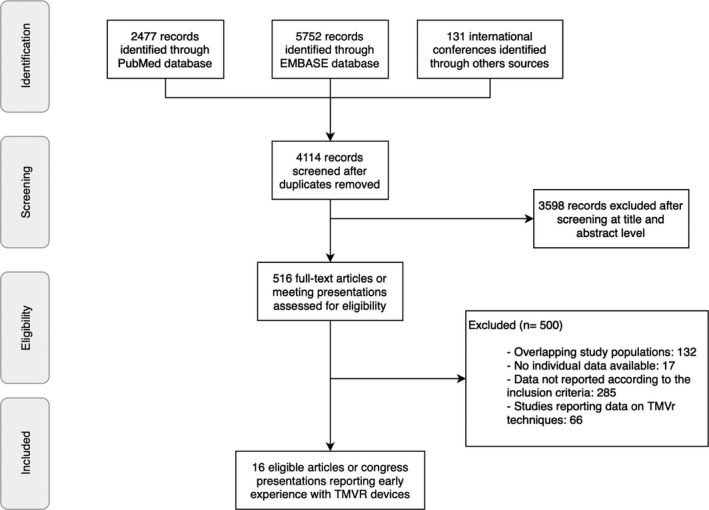
Background Transcatheter mitral valve replacement (TMVR) has emerged as an alternative therapeutic option for the treatment of severe mitral regurgitation in patients with prohibitive or high surgical risk. The aim of this systematic review is to evaluate the clinical procedural characteristics and outcomes associated with the early TMVR experience. Methods and Results Published studies and international conference presentations reporting data on TMVR systems were identified. Only records including clinical characteristics, procedural results, and 30-day and midterm outcomes were analyzed. A total of 16 publications describing 308 patients were analyzed. Most patients (65.9%) were men, with a mean age of 75 years (range: 69-81 years) and Society for Thoracic Surgery Predicted Risk of Mortality score of 7.7% (range: 6.1-8.6%). The etiology of mitral regurgitation was predominantly secondary or mixed (87.1%), and 81.5% of the patients were in New York Heart Association class III or IV. A transapical approach was used in 81.5% of patients, and overall technical success was high (91.7%). Postprocedural mean transmitral gradient was 3.5 mm Hg (range: 3-5.5 mm Hg), and only 4 cases (1.5%) presented residual moderate to severe mitral regurgitation. Procedural and all-cause 30-day mortality were 4.6% and 13.6%, respectively. Left ventricular outflow obstruction and conversion to open heart surgery were reported in 0.3% and 4% of patients, respectively. All-cause and cardiovascular-related mortality rates were 27.6% and 23.3%, respectively, after a mean follow-up of 10 (range: 3 to 24) months. Conclusions TMVR was a feasible, less invasive alternative for treating severe mitral regurgitation in patients with high or prohibitive surgical risk. TMVR was associated with a high rate of successful valve implantation and excellent hemodynamic results. However, periprocedural complications and all-cause mortality were relatively high.
Keywords: mitral valve disease; transcatheter cardiac therapeutics; transcatheter mitral valve replacement.
Figures
References
-
- Coffey S, Cairns BJ, Iung B. The modern epidemiology of heart valve disease. Heart. 2016;102:75–85. - PubMed
-
- Mirabel M, Iung B, Baron G, Messika‐Zeitoun D, Détaint D, Vanoverschelde J‐L, Butchart EG, Ravaud P, Vahanian A. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery? Eur Heart J. 2007;28:1358–1365. - PubMed
-
- Nishimura RA, Vahanian A, Eleid MF, Mack MJ. Mitral valve disease–current management and future challenges. Lancet. 2016;387:1324–1334. - PubMed
-
- Chiarito M, Pagnesi M, Martino EA, Pighi M, Scotti A, Biondi‐Zoccai G, Latib A, Landoni G, Mario CD, Margonato A, Maisano F, Feldman T, Alfieri O, Colombo A, Godino C. Outcome after percutaneous edge‐to‐edge mitral repair for functional and degenerative mitral regurgitation: a systematic review and meta‐analysis. Heart. 2018;104:306–312. - PubMed
-
- Regueiro A, Granada JF, Dagenais F, Rodés‐Cabau J. Transcatheter mitral valve replacement: insights from early clinical experience and future challenges. J Am Coll Cardiol. 2017;69:2175–2192. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
